

Large scale genotype-phenotype analyses indicate that novel prognostic tools are required for families with facioscapulohumeral muscular dystrophy
- PMID: 24030947
- PMCID: PMC3808686
- DOI: 10.1093/brain/awt226
Large scale genotype-phenotype analyses indicate that novel prognostic tools are required for families with facioscapulohumeral muscular dystrophy
Abstract
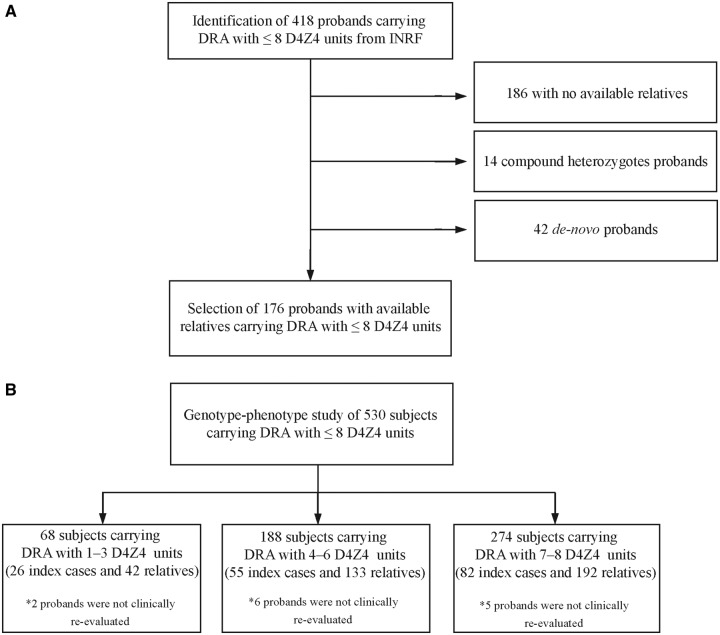
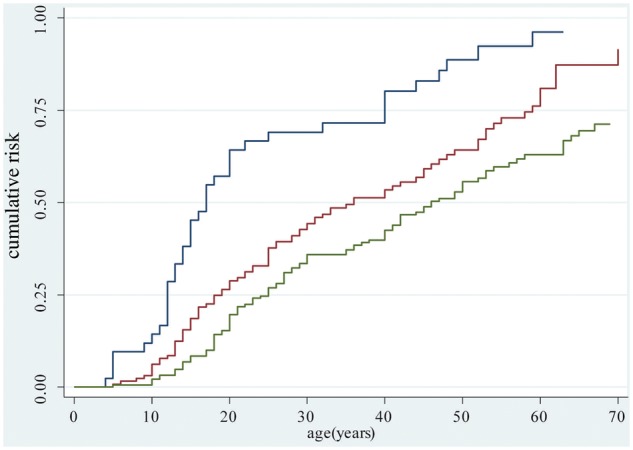
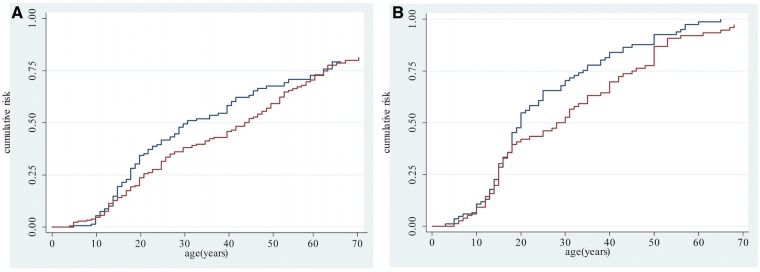
Facioscapulohumeral muscular dystrophy has been genetically linked to reduced numbers (≤ 8) of D4Z4 repeats at 4q35 combined with 4A(159/161/168) DUX4 polyadenylation signal haplotype. However, we have recently reported that 1.3% of healthy individuals carry this molecular signature and 19% of subjects affected by facioscapulohumeral muscular dystrophy do not carry alleles with eight or fewer D4Z4 repeats. Therefore, prognosis for subjects carrying or at risk of carrying D4Z4 reduced alleles has become more complicated. To test for additional prognostic factors, we measured the degree of motor impairment in a large group of patients affected by facioscapulohumeral muscular dystrophy and their relatives who are carrying D4Z4 reduced alleles. The clinical expression of motor impairment was assessed in 530 subjects, 163 probands and 367 relatives, from 176 unrelated families according to a standardized clinical score. The associations between clinical severity and size of D4Z4 allele, degree of kinship, gender, age and 4q haplotype were evaluated. Overall, 32.2% of relatives did not display any muscle functional impairment. This phenotype was influenced by the degree of relation with proband, because 47.1% of second- through fifth-degree relatives were unaffected, whereas only 27.5% of first-degree family members did not show motor impairment. The estimated risk of developing motor impairment by age 50 for relatives carrying a D4Z4 reduced allele with 1-3 repeats or 4-8 repeats was 88.7% and 55%, respectively. Male relatives had a mean score significantly higher than females (5.4 versus 4.0, P = 0.003). No 4q haplotype was exclusively associated with the presence of disease. In 13% of families in which D4Z4 alleles with 4-8 repeats segregate, the diagnosis of facioscapulohumeral muscular dystrophy was reported only in one generation. In conclusion, this large-scale analysis provides further information that should be taken into account when counselling families in which a reduced allele with 4-8 D4Z4 repeats segregates. In addition, the reduced expression of disease observed in distant relatives suggests that a family's genetic background plays a role in the occurrence of facioscapulohumeral muscular dystrophy. These results indicate that the identification of new susceptibility factors for this disease will require an accurate classification of families.
Keywords: D4Z4 reduced allele; disease expression; facioscapulohumeral muscular dystrophy; genotype–phenotype correlations; penetrance.
Figures

References
-
- Flanigan KM. Facioscapulohumeral muscular dystrophy and scapulohumeral syndrome. In: Engel AG, Franzini-Armstrong C, editors. Myology. New York: McGraw-Hill; 2004. pp. 123–34.
-
- Griggs RC, Tawil R, Storvick D, Mendell JR, Altherr MR. Genetics of facioscapulohumeral muscular dystrophy: new mutations in sporadic cases. Neurology. 1993;43:2369–72. - PubMed
-
- Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–81.
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
