

Early detection of liver steatosis by magnetic resonance imaging in rats infused with glucose and intralipid solutions and correlation to insulin levels
- PMID: 24035445
- PMCID: PMC3914148
- DOI: 10.1016/j.metabol.2013.08.003
Early detection of liver steatosis by magnetic resonance imaging in rats infused with glucose and intralipid solutions and correlation to insulin levels
Abstract
Objective: Magnetic resonance (MR) techniques allow noninvasive fat quantification. We aimed to investigate the accuracy of MR imaging (MRI), MR spectroscopy (MRS) and histological techniques to detect early-onset liver steatosis in three rat phenotypes assigned to an experimental glucolipotoxic model or a control group.
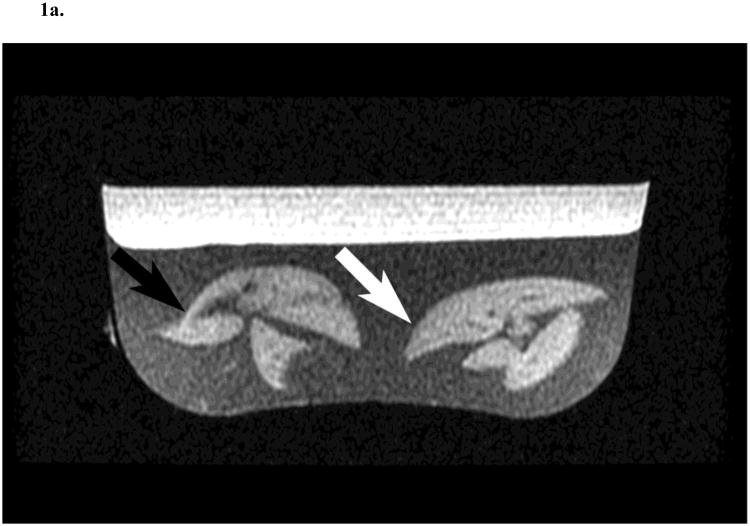
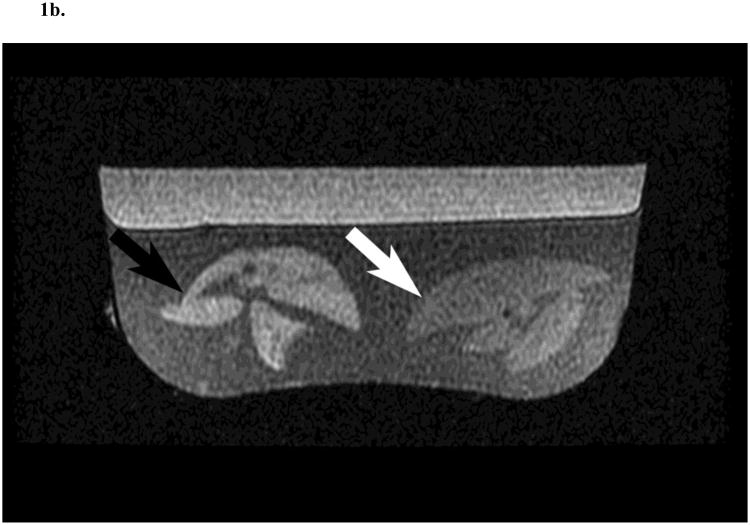
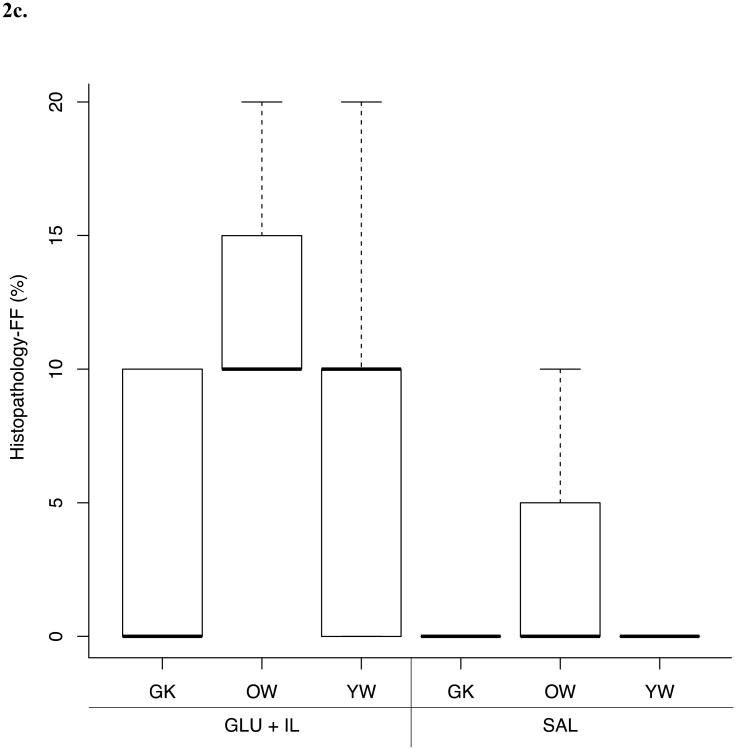
Materials and methods: This study was approved by the institutional committee for the protection of animals. Thirty-two rats (13 young Wistar, 6 old Wistar and 13 diabetic Goto-Kakizaki rats) fed a standard diet were assigned to a 72h intravenous infusion of glucose and Intralipid fat emulsion or a saline infusion. Plasma insulin levels were measured. Steatosis was quantified in ex vivo livers with gradient-recalled multi-echo MRI, MRS and histology as fat fractions (FF).
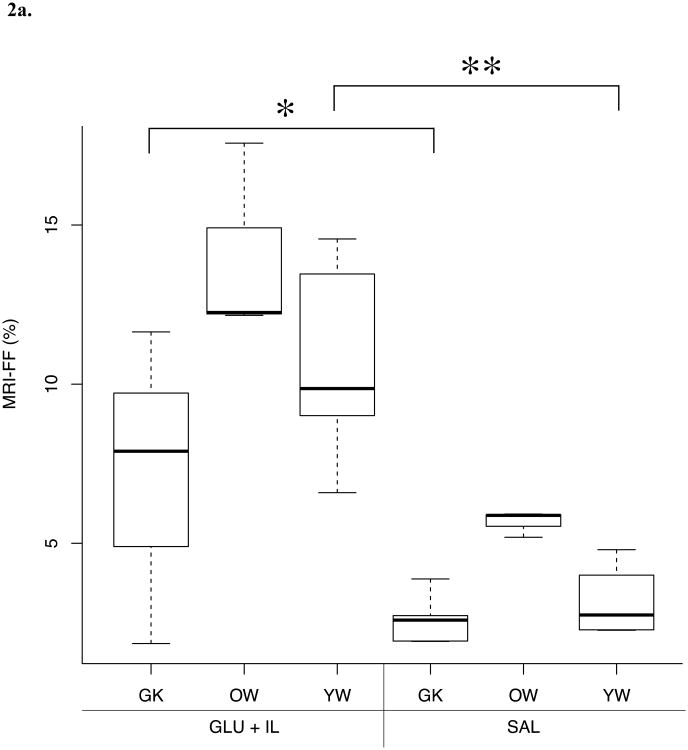
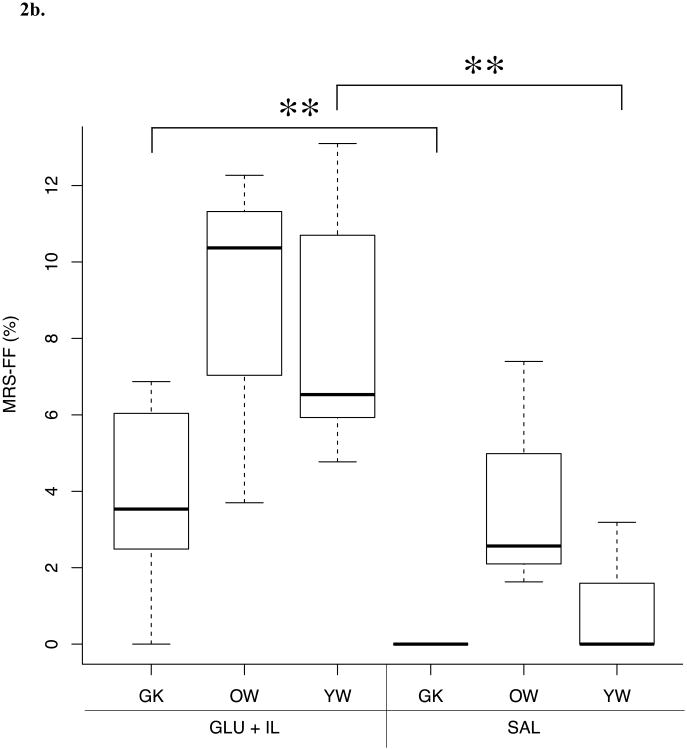
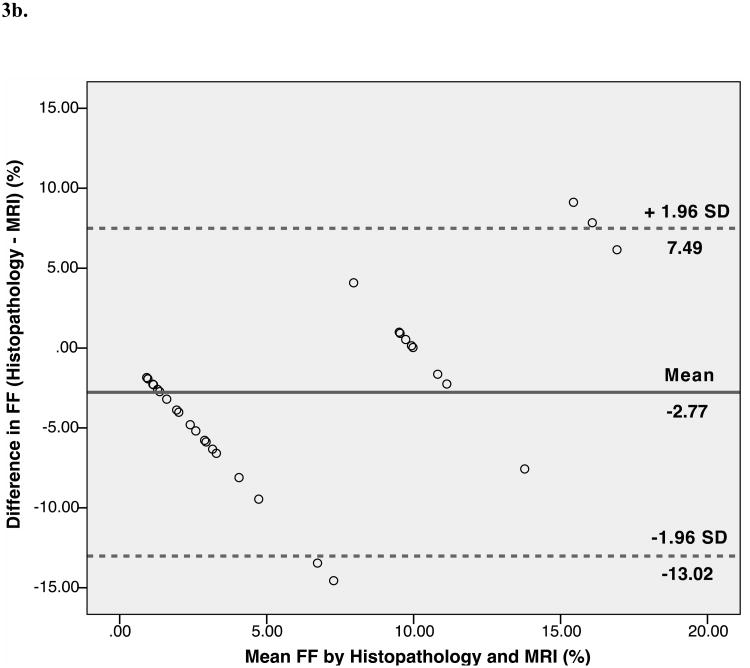
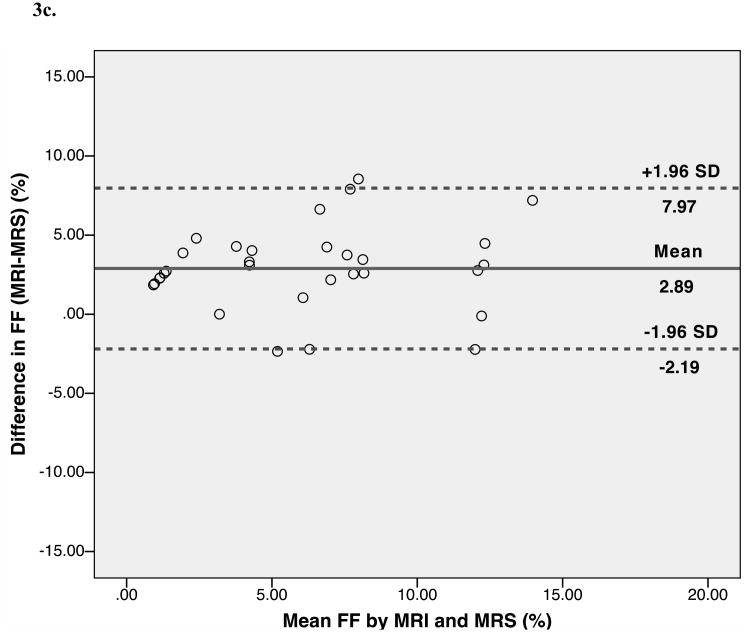
Results: A significant correlation was found between multi-echo MRI-FF and MRS-FF (r=0.81, p<0.01) and a weaker correlation was found between histology and MRS-FF (r=0.60, p<0.01). MRS and MRI accurately distinguished young Wistar and Goto-Kakizaki rats receiving the glucose+Intralipid infusion from those receiving the saline control whereas histology did not. Significant correlations were found between MRI or MRS and insulin plasma level (r=0.63, p<0.01; r=0.57, p<0.01), and between MRI or MRS and C-peptide concentration (r=0.54, p<0.01; r=0.44, p<0.02).
Conclusions: Multi-echo MRI and MRS may be more sensitive to measure early-onset liver steatosis than histology in an experimental glucolipotoxic rat model.
Keywords: Diabetes mellitus; FF; Fat fraction; GLU+IL; Glucose+Intralipid; Hepatic steatosis; IP; In-phase; Insulin; MR; MRI; MRS; Magnetic resonance; Magnetic resonance imaging; Magnetic resonance spectroscopy; NAFLD; NASH; Nonalcoholic fatty liver disease; Nonalcoholic steatohepatitis; OP; Opposed-phase; ROC; Receiver operating characteristic; SAL; Saline.
© 2013.
Conflict of interest statement
Figures

References
-
- Shibata M, Kihara Y, Taguchi M, et al. Nonalcoholic fatty liver disease is a risk factor for type 2 diabetes in middle-aged japanese men. Diabetes Care. 2007;30(11):2940–4. - PubMed
-
- Kotronen A, Juurinen L, Hakkarainen A, et al. Liver fat is increased in type 2 diabetic patients and underestimated by serum alanine aminotransferase compared with equally obese nondiabetic subjects. Diabetes Care. 2008;31(1):165–9. - PubMed
-
- Younossi ZM, Otgonsuren M, Venkatesan C, et al. In patients with non-alcoholic fatty liver disease, metabolically abnormal individuals are at a higher risk for mortality while metabolically normal individuals are not. Metabolism. 2013;62(3):352–60. - PubMed
-
- Adams LA, Talwalkar JA. Diagnostic evaluation of nonalcoholic fatty liver disease. J Clin Gastroenterol. 2006;40(3 Suppl 1):S34–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
