

Intracoronary cardiosphere-derived cells after myocardial infarction: evidence of therapeutic regeneration in the final 1-year results of the CADUCEUS trial (CArdiosphere-Derived aUtologous stem CElls to reverse ventricUlar dySfunction)
- PMID: 24036024
- PMCID: PMC3947063
- DOI: 10.1016/j.jacc.2013.08.724
Intracoronary cardiosphere-derived cells after myocardial infarction: evidence of therapeutic regeneration in the final 1-year results of the CADUCEUS trial (CArdiosphere-Derived aUtologous stem CElls to reverse ventricUlar dySfunction)
Abstract
Objectives: This study sought to report full 1-year results, detailed magnetic resonance imaging analysis, and determinants of efficacy in the prospective, randomized, controlled CADUCEUS (CArdiosphere-Derived aUtologous stem CElls to reverse ventricUlar dySfunction) trial.
Background: Cardiosphere-derived cells (CDCs) exerted regenerative effects at 6 months in the CADUCEUS trial. Complete results at the final 1-year endpoint are unknown.
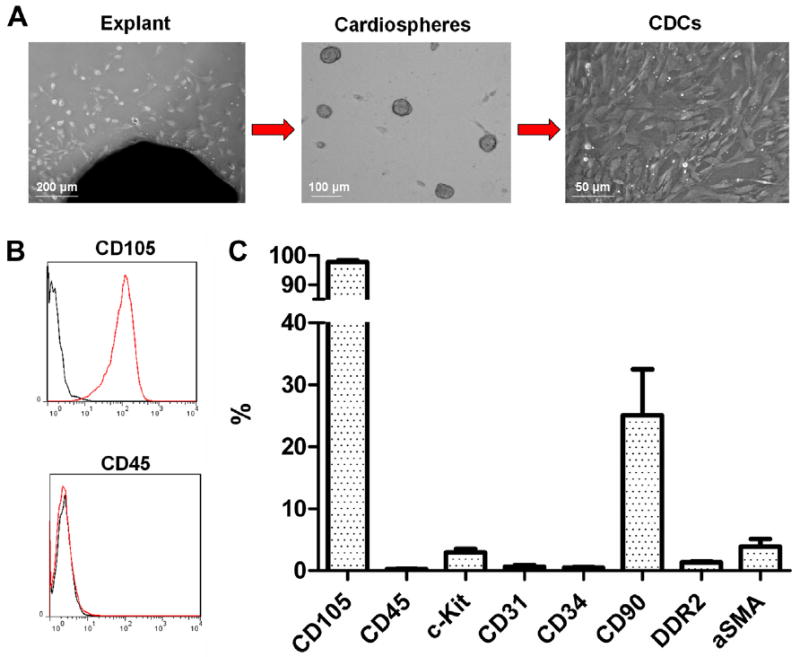
Methods: Autologous CDCs (12.5 to 25 × 10(6)) grown from endomyocardial biopsy specimens were infused via the intracoronary route in 17 patients with left ventricular dysfunction 1.5 to 3 months after myocardial infarction (MI) (plus 1 infused off-protocol 14 months post-MI). Eight patients were followed as routine-care control patients.
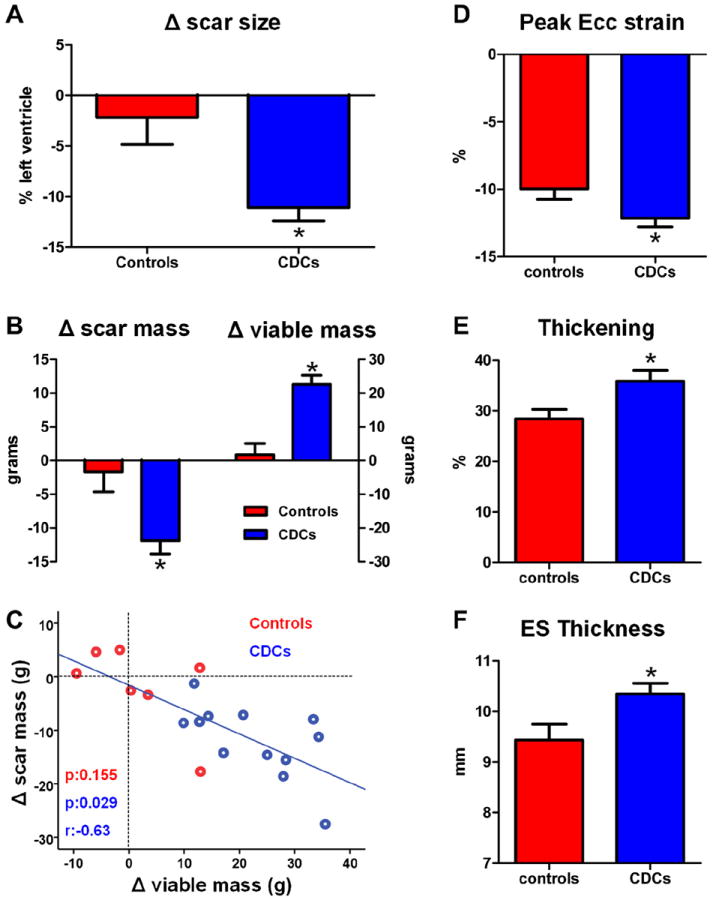
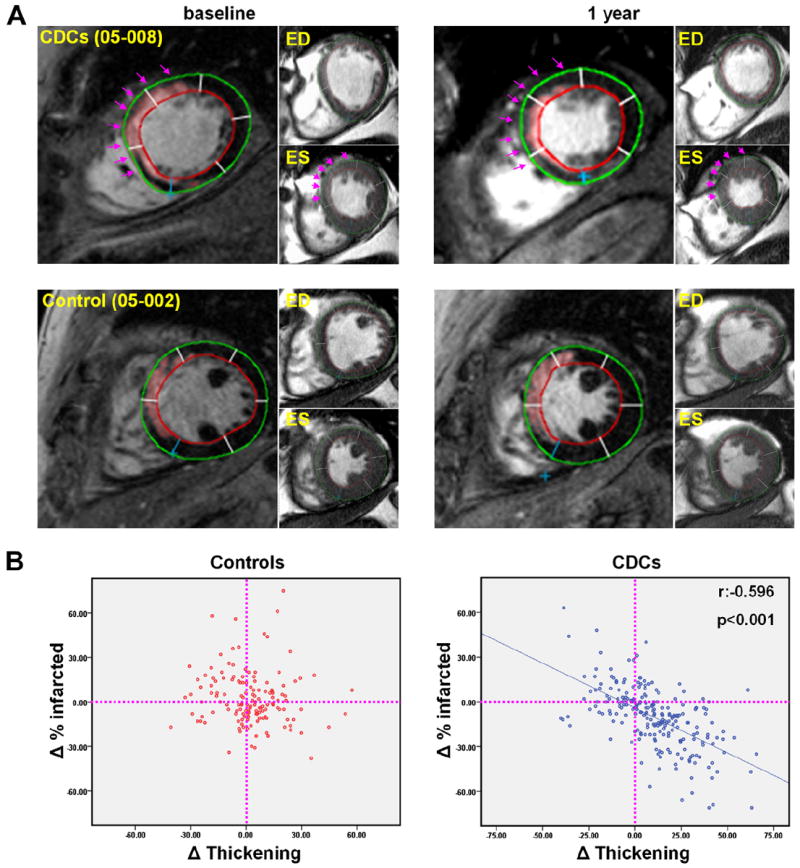
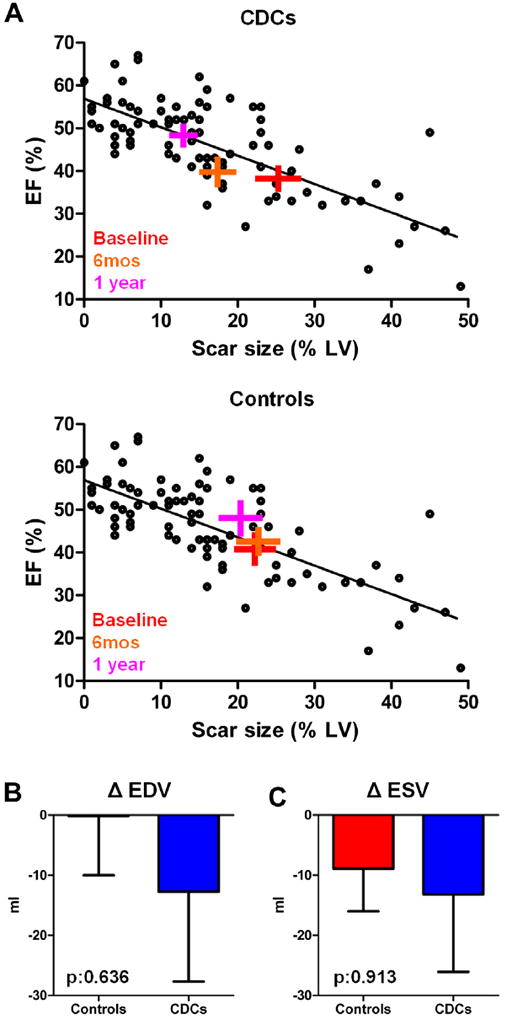
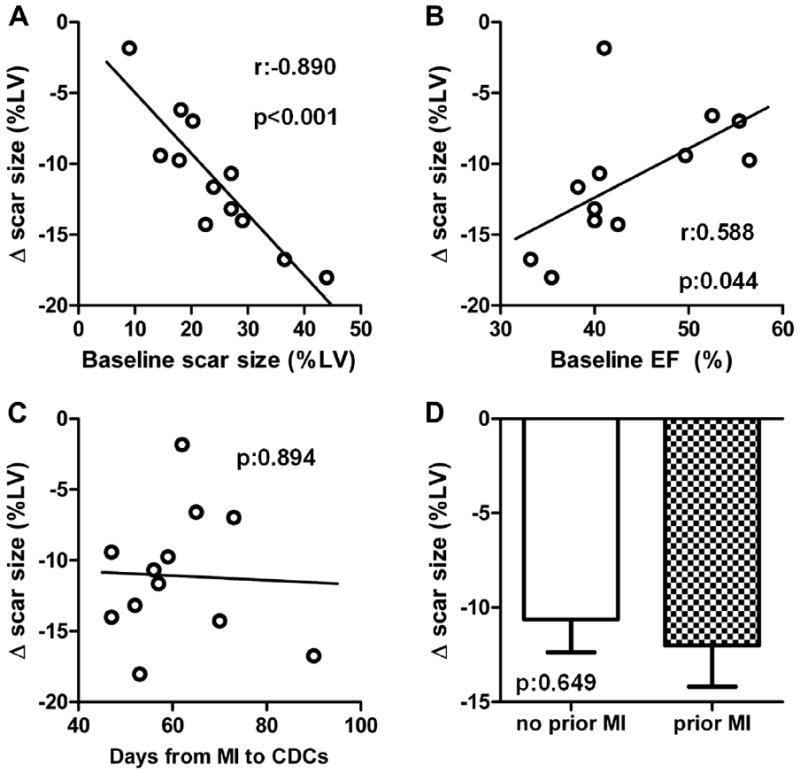
Results: In 13.4 months of follow-up, safety endpoints were equivalent between groups. At 1 year, magnetic resonance imaging revealed that CDC-treated patients had smaller scar size compared with control patients. Scar mass decreased and viable mass increased in CDC-treated patients but not in control patients. The single patient infused 14 months post-MI responded similarly. CDC therapy led to improved regional function of infarcted segments compared with control patients. Scar shrinkage correlated with an increase in viability and with improvement in regional function. Scar reduction correlated with baseline scar size but not with a history of temporally remote MI or time from MI to infusion. The changes in left ventricular ejection fraction in CDC-treated subjects were consistent with the natural relationship between scar size and ejection fraction post-MI.
Conclusions: Intracoronary administration of autologous CDCs did not raise significant safety concerns. Preliminary indications of bioactivity include decreased scar size, increased viable myocardium, and improved regional function of infarcted myocardium at 1 year post-treatment. These results, which are consistent with therapeutic regeneration, merit further investigation in future trials. (CArdiosphere-Derived aUtologous stem CElls to reverse ventricUlar dySfunction [CADUCEUS]; NCT00893360).
Keywords: CDC; CK-MB; CT; DSMB; Data and Safety Monitoring Board; EDV; EF; ESV; Ecc; FWHM; ICD; LV; LVEF; MI; MRI; NYHA; New York Heart Association; SAE; TnI; Vo(2); cardiosphere-derived cell; cardiosphere-derived cells; computed tomography; creatine kinase-myocardial band; ejection fraction; end-diastolic volume; end-systolic volume; full width at half maximum; implantable cardioverter-defibrillator; left ventricular; left ventricular ejection fraction; magnetic resonance imaging; myocardial infarction; myocardial regeneration; oxygen consumption; serious adverse event(s); systolic circumferential strain; troponin I.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. 2007;356:2388–98. - PubMed
-
- White HD, Aylward PE, Huang Z, et al. VALIANT Investigators. Mortality and morbidity remain high despite captopril and/or Valsartan therapy in elderly patients with left ventricular systolic dysfunction, heart failure, or both after acute myocardial infarction: results from the Valsartan in Acute Myocardial Infarction Trial (VALIANT) Circulation. 2005;112:3391–9. - PubMed
-
- Janssens S, Dubois C, Bogaert J, et al. Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevation myocardial infarction: double-blind, randomised controlled trial. Lancet. 2006;367:113–21. - PubMed
-
- Lunde K, Solheim S, Aakhus S, et al. Intracoronary injection of mononuclear bone marrow cells in acute myocardial infarction. N Engl J Med. 2006;355:1199–209. - PubMed
-
- Meyer GP, Wollert KC, Lotz J, et al. Intracoronary bone marrow cell transfer after myocardial infarction: eighteen months’ follow-up data from the randomized, controlled BOOST (BOne marrOw transfer to enhance ST-elevation infarct regeneration) trial. Circulation. 2006;113:1287–94. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
