

Evaluation of the influence of tumor location and size on the difference of dose calculation between Ray Tracing algorithm and Fast Monte Carlo algorithm in stereotactic body radiotherapy of non-small cell lung cancer using CyberKnife
- PMID: 24036860
- PMCID: PMC5714561
- DOI: 10.1120/jacmp.v14i5.4280
Evaluation of the influence of tumor location and size on the difference of dose calculation between Ray Tracing algorithm and Fast Monte Carlo algorithm in stereotactic body radiotherapy of non-small cell lung cancer using CyberKnife
Abstract
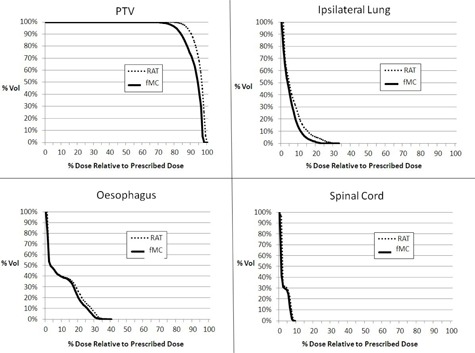
This study evaluated the extent of improvement in dose predication accuracy achieved by the Fast Monte Carlo algorithm (MC) compared to the Ray Tracing algorithm (RAT) in stereotactic body radiotherapy (SBRT) of non-small cell lung cancer (NSCLC), and how their differences were influenced by the tumor site and size. Thirty-three NSCLC patients treated with SBRT by CyberKnife in 2011 were recruited. They were divided into the central target group (n = 17) and peripheral target group (n = 16) according to the RTOG 0236 guidelines. Each group was further divided into the large and small target subgroups. After the computation of treatment plans using RAT, a MC plan was generated using the same patient data and treatment parameters. Apart from the target reference point dose measurements, various dose parameters for the planning target volume (PTV) and organs at risk (OARs) were assessed. In addition, the "Fractional Deviation" (FDev) was also calculated for comparison, which was defined as the ratio of the RAT and MC values. For peripheral lung cases, RAT produced significantly higher dose values in all the reference points than MC. The FDev of all reference point doses and dose parameters was greater in the small target than the large target subgroup. For central lung cases, there was no significant reference point and OAR dose differences between RAT and MC. When comparing between the small target and large target subgroups, the FDev values of all the dose parameters and reference point doses did not show significant difference. Despite the shorter computation time, RAT was inferior to MC, in which the target dose was usually overestimated. RAT would not be recommended for SBRT of peripheral lung tumors regardless of the target size. However, it could be considered for large central lung tumors because its performance was comparable to MC.
Figures



References
-
- Brown WT, Wu X, Fayad F, et al. Application of robotic stereotactic radiotherapy to peripheral stage I non‐small cell lung cancer with curative intent. Clin Oncol. 2009;21(8):623–31. - PubMed
-
- van der Voort van Zyp NC, Prvost J, Hoogeman MS, et al. Stereotactic radiotherapy with real‐time tumor tracking for non‐small cell lung cancer: clinical outcome. Radiother Oncol. 2009;91(3):296–300. - PubMed
-
- Timmerman R, McGarry R, Yiannoutsos C, et al. Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inoperable early‐stage lung cancer. J Clin Oncol. 2006;24(30):4833–39. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
