

Application of failure mode and effects analysis (FMEA) to pretreatment phases in tomotherapy
- PMID: 24036868
- PMCID: PMC5714567
- DOI: 10.1120/jacmp.v14i5.4329
Application of failure mode and effects analysis (FMEA) to pretreatment phases in tomotherapy
Abstract
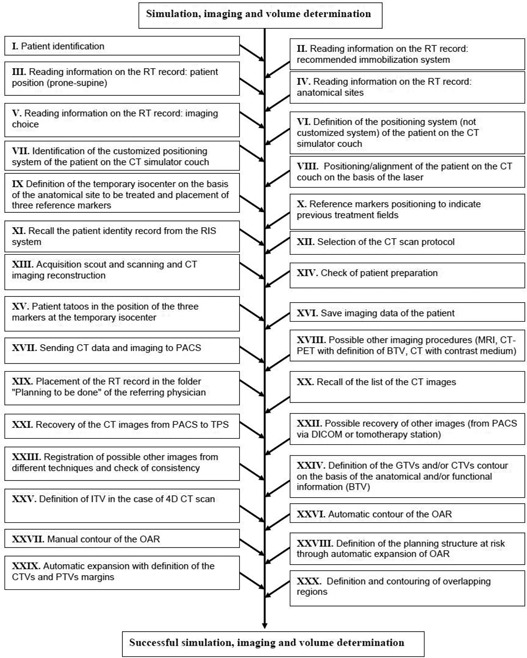
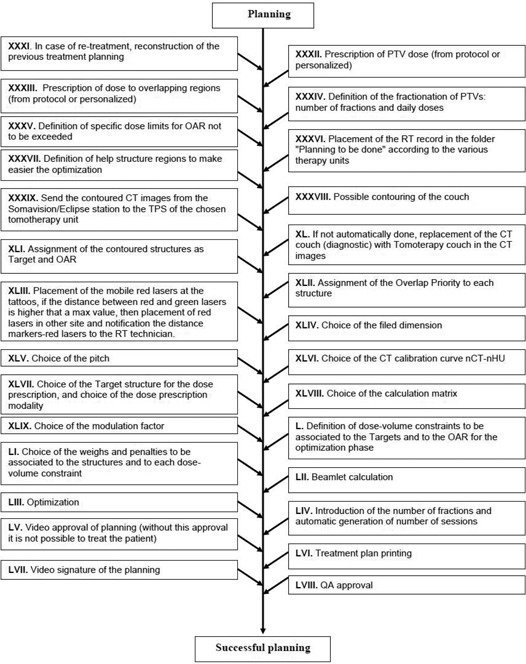
The aim of this paper was the application of the failure mode and effects analysis (FMEA) approach to assess the risks for patients undergoing radiotherapy treatments performed by means of a helical tomotherapy unit. FMEA was applied to the preplanning imaging, volume determination, and treatment planning stages of the tomotherapy process and consisted of three steps: 1) identification of the involved subprocesses; 2) identification and ranking of the potential failure modes, together with their causes and effects, using the risk probability number (RPN) scoring system; and 3) identification of additional safety measures to be proposed for process quality and safety improvement. RPN upper threshold for little concern of risk was set at 125. A total of 74 failure modes were identified: 38 in the stage of preplanning imaging and volume determination, and 36 in the stage of planning. The threshold of 125 for RPN was exceeded in four cases: one case only in the phase of preplanning imaging and volume determination, and three cases in the stage of planning. The most critical failures appeared related to (i) the wrong or missing definition and contouring of the overlapping regions, (ii) the wrong assignment of the overlap priority to each anatomical structure, (iii) the wrong choice of the computed tomography calibration curve for dose calculation, and (iv) the wrong (or not performed) choice of the number of fractions in the planning station. On the basis of these findings, in addition to the safety strategies already adopted in the clinical practice, novel solutions have been proposed for mitigating the risk of these failures and to increase patient safety.
Figures
References
-
- Hoeschen C, Mattsson S, Cantone MC, et al. Minimising activity and dose with enhanced image quality by radiopharmaceutical administrations. Rad Prot Dosimetry. 2010;139(1–3):250–53. - PubMed
-
- Mancosu P, Cozzi L, Fogliata A, et al. Collimator angle influence on dose distribution optimization for vertebral metastases using volumetric modulated arc therapy. Med Phys. 2010;37(8):4133–37. - PubMed
-
- Korreman S, Rasch C, McNair H, et al. The European Society of Therapeutic Radiology and Oncology‐European Institute of Radiotherapy (ESTRO‐EIR) report on 3D CT‐based in‐room image guidance systems: a practical and technical review and guide. Radiother Oncol. 2010;94(2):129–44. - PubMed
-
- Broggi S, Cattaneo GM, Molinelli S, et al. Results of a two‐year quality control program for a helical tomotherapy unit. Radiother Oncol. 2008;86(2):231–41. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
