

The impact of out-of-pocket costs on the use of intrauterine contraception among women with employer-sponsored insurance
- PMID: 24036995
- PMCID: PMC6702955
- DOI: 10.1097/MLR.0b013e3182a97b5d
The impact of out-of-pocket costs on the use of intrauterine contraception among women with employer-sponsored insurance
Abstract
Background: Long-acting reversible contraception (LARC) is highly effective but also has higher initiation costs than oral contraceptive methods, which may contribute to relatively low use. The Affordable Care Act requires most private insurance plans to cover contraceptive services without patient cost-sharing. Whether this mandate will increase LARC use is unknown.
Objective: To assess the relationship between cost-sharing and use of LARC among privately insured women.
Design: Cross-sectional analysis using Truven Health MarketScan data from January 2011 to December 2011.
Subjects: Women aged 14-45 years with continuous insurance coverage enrolled in health plan products that covered branded and generic oral contraceptive pills (OCPs) and intrauterine devices (IUDs). We selected women using OCPs and IUDs as these are the most commonly used short-acting and long-acting reversible methods, respectively (N=1,682,425).
Measures: Multivariable regression was used to assess the association of the level of out-of-pocket costs for IUDs for each patient's plan and IUD initiation, adjusting for out-of-pocket costs for branded and generic OCPs and patient characteristics.
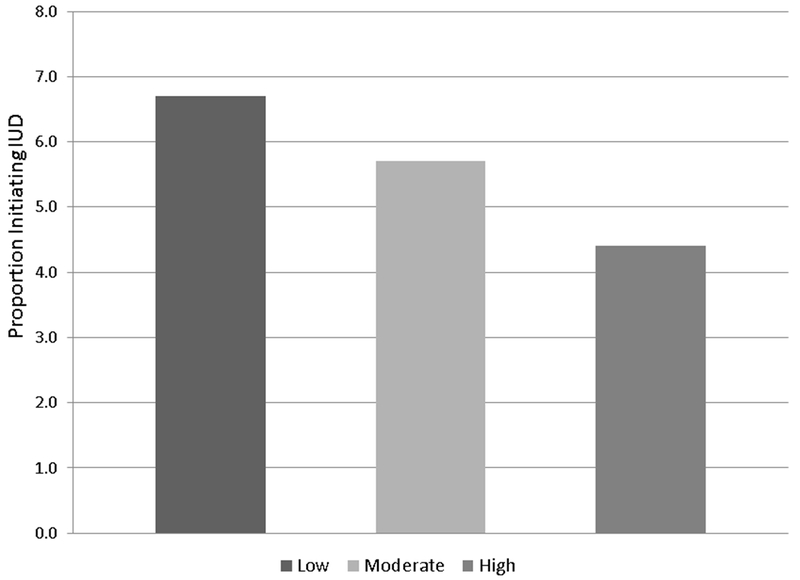
Results: Overall, 5.5% of women initiated an IUD in 2011. After adjustment, IUD initiation was less likely among women with higher versus lower co-pays (adjusted risk ratio=0.65; 95% CI, 0.64-0.67). Women who saw an obstetrician/gynecologist during 2011 were more likely to initiate an IUD (adjusted risk ratio=2.49; 95% CI, 2.45-2.53).
Conclusions: Rates of IUD use are low among privately insured women in the United States, and higher cost-sharing is associated with lower rates of IUD use. Together with other measures to promote LARC use, eliminating co-pays for contraception could promote the use of these more effective and cost-effective methods.
Figures
Similar articles
-
Cost Sharing and Utilization of Postpartum Intrauterine Devices and Contraceptive Implants Among Commercially Insured Women.Womens Health Issues. 2019 Nov-Dec;29(6):465-470. doi: 10.1016/j.whi.2019.07.006. Epub 2019 Sep 5. Womens Health Issues. 2019. PMID: 31495642
-
Early Impact of the Affordable Care Act on Uptake of Long-acting Reversible Contraceptive Methods.Med Care. 2016 Sep;54(9):811-7. doi: 10.1097/MLR.0000000000000551. Med Care. 2016. PMID: 27213549 Free PMC article.
-
Cost sharing, postpartum contraceptive use, and short interpregnancy interval rates among commercially insured women.Am J Obstet Gynecol. 2021 Mar;224(3):282.e1-282.e17. doi: 10.1016/j.ajog.2020.08.109. Epub 2020 Sep 6. Am J Obstet Gynecol. 2021. PMID: 32898503
-
Canadian Contraception Consensus (Part 1 of 4).J Obstet Gynaecol Can. 2015 Oct;37(10):936-42. doi: 10.1016/s1701-2163(16)30033-0. J Obstet Gynaecol Can. 2015. PMID: 26606712 English, French.
-
Intrauterine devices. The optimal long-term contraceptive method?J Reprod Med. 1999 Mar;44(3):269-74. J Reprod Med. 1999. PMID: 10202746 Review.
Cited by
-
The Association between High-Deductible Health Plan Transition and Contraception and Birth Rates.Health Serv Res. 2016 Feb;51(1):187-204. doi: 10.1111/1475-6773.12326. Epub 2015 Jun 29. Health Serv Res. 2016. PMID: 26118959 Free PMC article.
-
Women's Contraceptive Preference-Use Mismatch.J Womens Health (Larchmt). 2017 Jun;26(6):692-701. doi: 10.1089/jwh.2016.5807. Epub 2016 Oct 6. J Womens Health (Larchmt). 2017. PMID: 27710196 Free PMC article.
-
Iran's Health System Transformation Plan: A SWOT analysis.Med J Islam Repub Iran. 2018 May 12;32:39. doi: 10.14196/mjiri.32.39. eCollection 2018. Med J Islam Repub Iran. 2018. PMID: 30159290 Free PMC article.
-
Reducing Unintended Pregnancies Through Web-Based Reproductive Life Planning and Contraceptive Action Planning among Privately Insured Women: Study Protocol for the MyNewOptions Randomized, Controlled Trial.Womens Health Issues. 2015 Nov-Dec;25(6):641-8. doi: 10.1016/j.whi.2015.06.010. Epub 2015 Aug 22. Womens Health Issues. 2015. PMID: 26307564 Free PMC article. Clinical Trial.
-
Changes to Contraceptive Method Use at Title X Clinics Following Delaware Contraceptive Access Now, 2008-2017.Am J Public Health. 2020 Aug;110(8):1214-1220. doi: 10.2105/AJPH.2020.305666. Epub 2020 Jun 18. Am J Public Health. 2020. PMID: 32552027 Free PMC article.
References
-
- Department of HHS. News Release: Affordable Care Act Ensures Women Receive Preventive Services at No Additional Cost. 2011. http://www.hhs.gov/news/press/2011pres/08/20110801b.html. Accessed March 18, 2013.
-
- Dennis A, Grossman D. Barriers to Contraception and Interest In Over-the-Counter Access Among Low-Income Women: A Qualitative Study. Perspect Sex Reprod Health. June 2012;44(2):84–91. - PubMed
-
- Thompson KM, Speidel JJ, Saporta V, Waxman NJ, Harper CC. Contraceptive policies affect post-abortion provision of long-acting reversible contraception. Contraception. January 2011;83(1):41–47. - PubMed
-
- Magnusson BM, Sabik L, Chapman DA, et al. Contraceptive insurance mandates and consistent contraceptive use among privately insured women. Med Care. July 2012;50(7):562–568. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
