

Sinonasal tract and nasopharyngeal adenoid cystic carcinoma: a clinicopathologic and immunophenotypic study of 86 cases
- PMID: 24037641
- PMCID: PMC3950387
- DOI: 10.1007/s12105-013-0487-3
Sinonasal tract and nasopharyngeal adenoid cystic carcinoma: a clinicopathologic and immunophenotypic study of 86 cases
Abstract
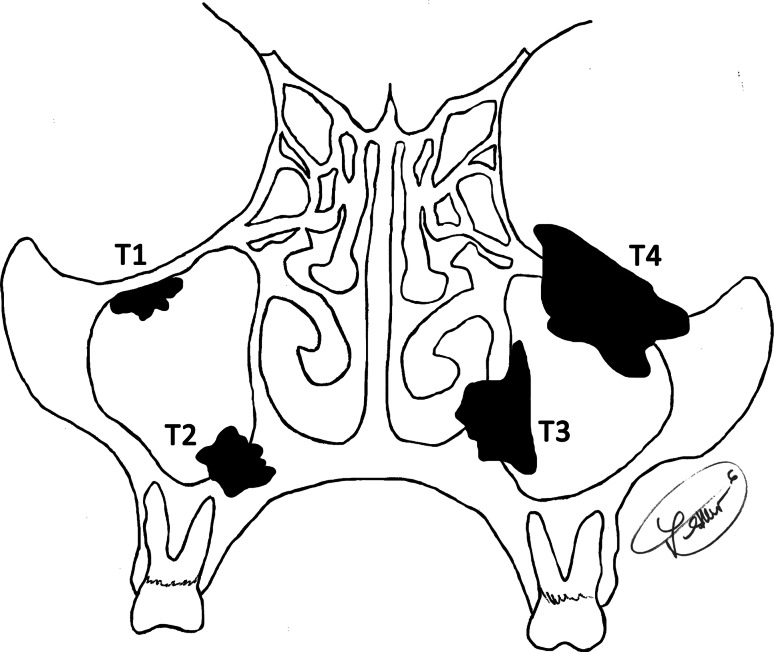
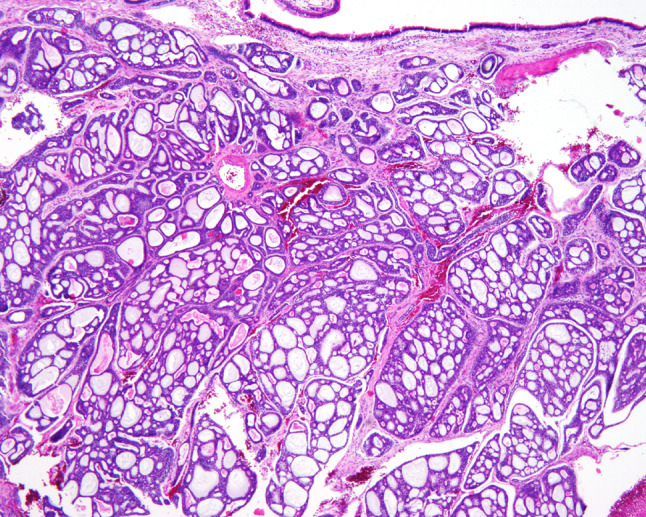
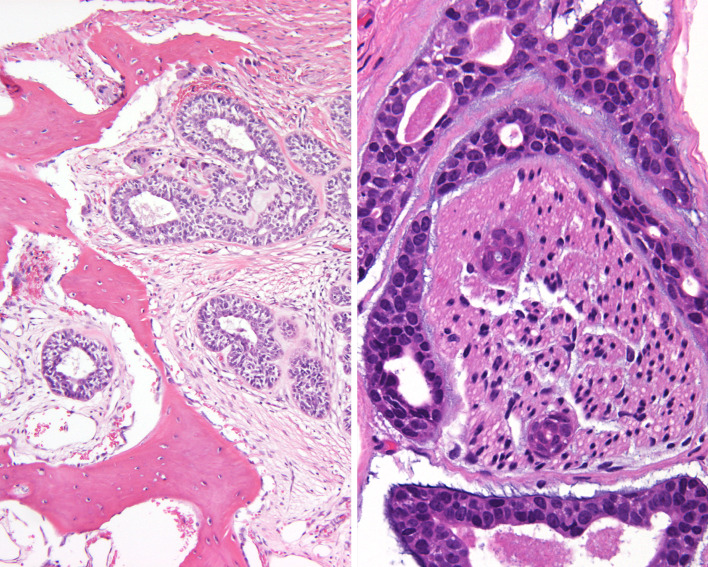
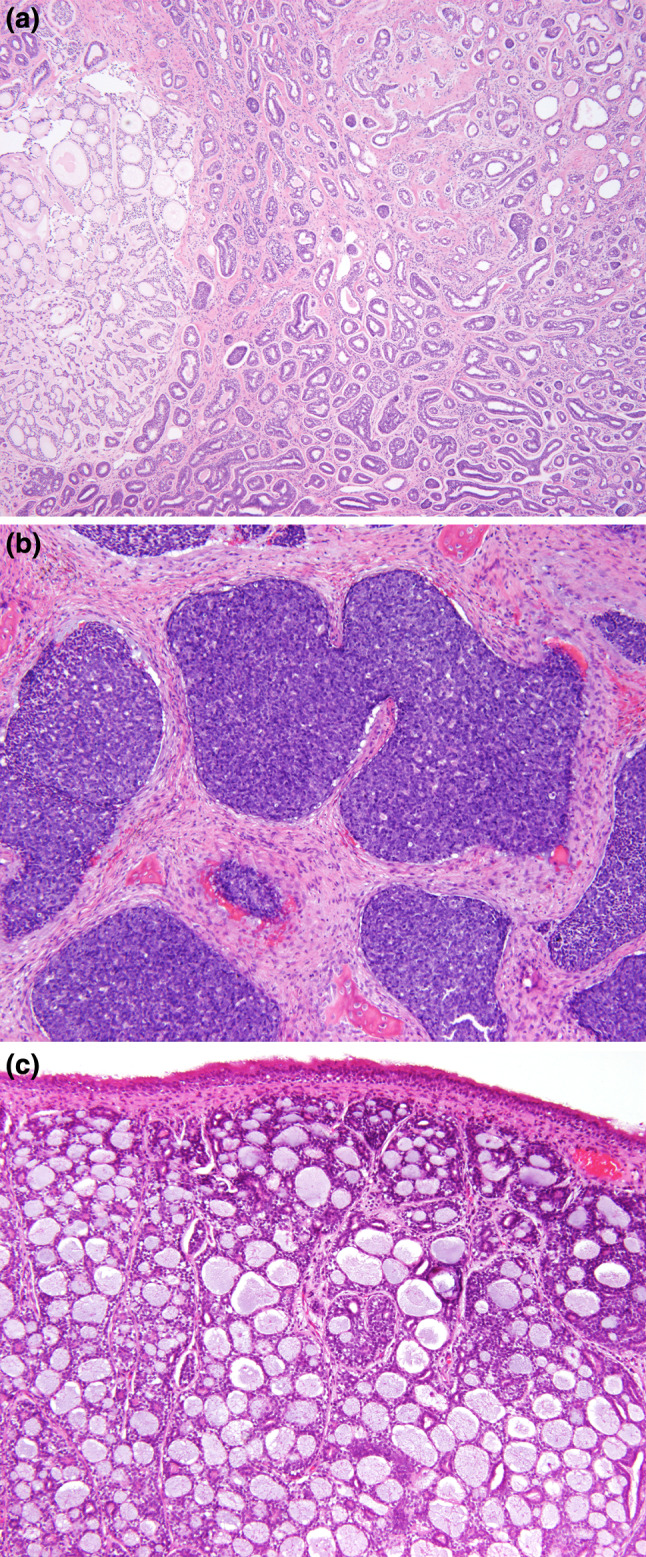
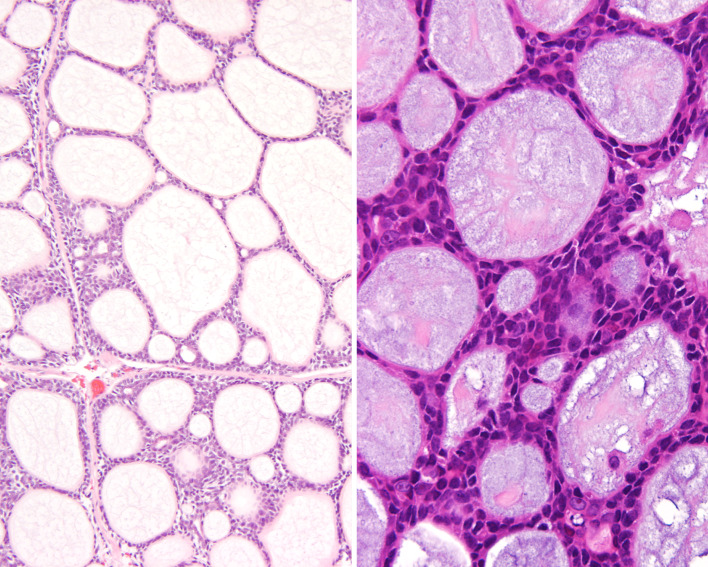
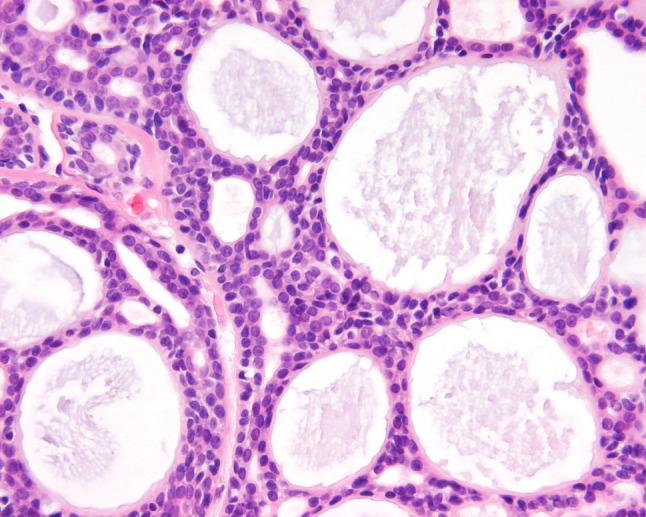
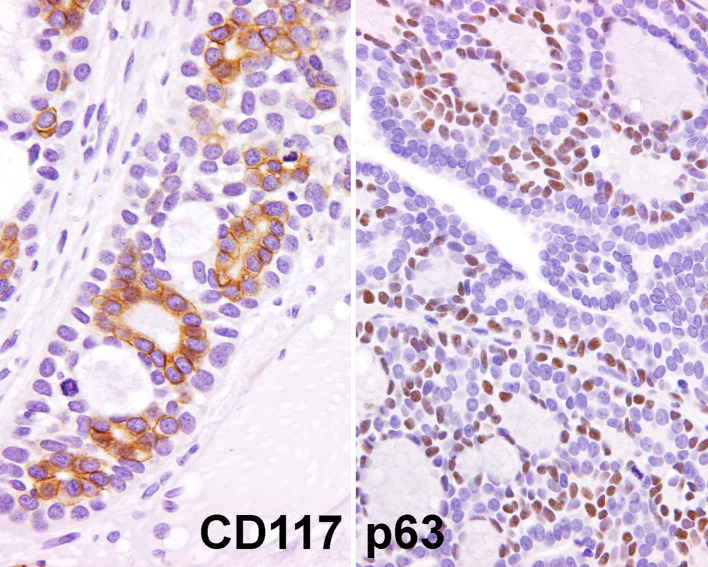
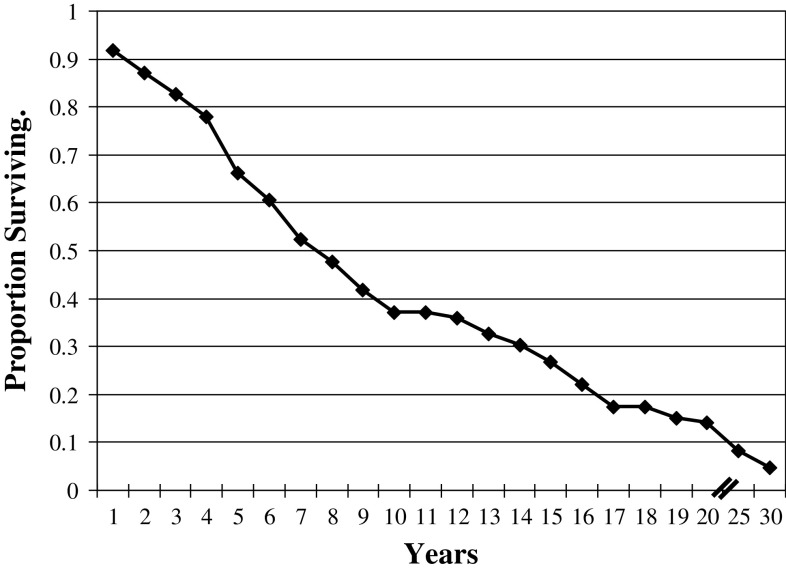
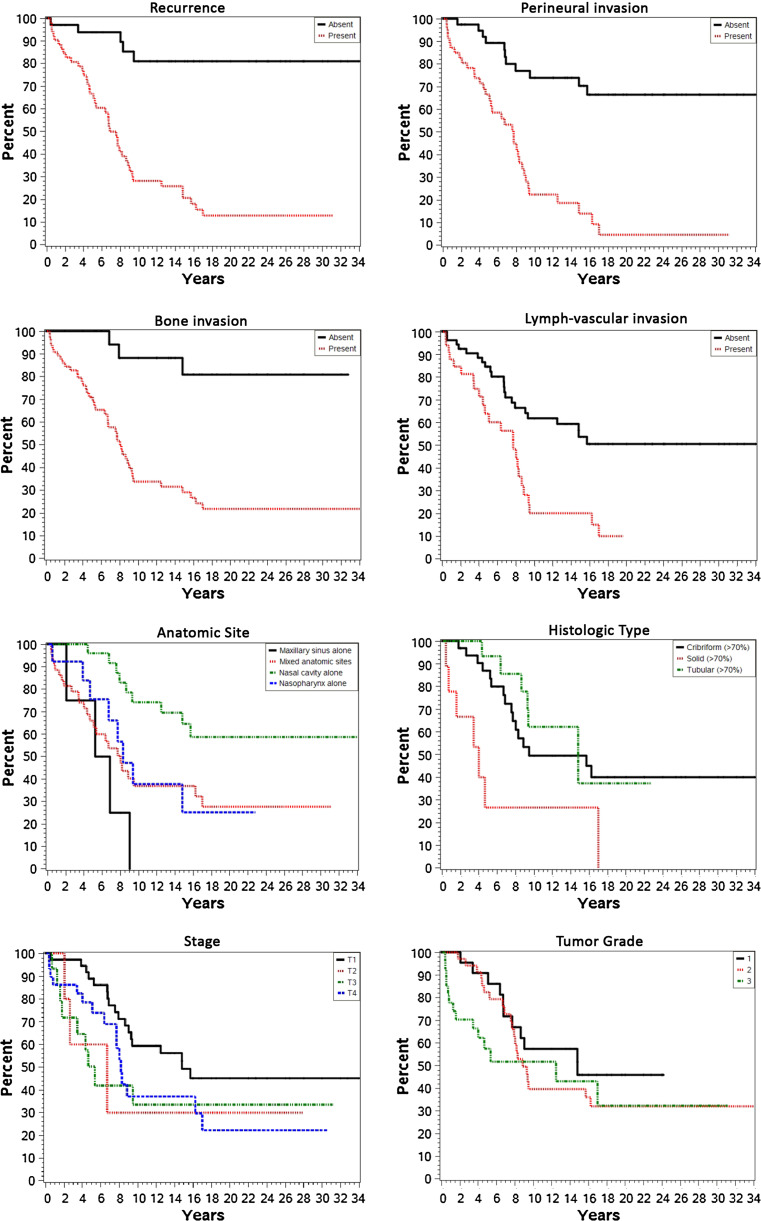
Primary sinonasal tract and nasopharyngeal adenoid cystic carcinomas (STACC) are uncommon tumors that are frequently misclassified, resulting in inappropriate clinical management. Eighty-six cases of STACC included 45 females and 41 males, aged 12-91 years (mean 54.4 years). Patients presented most frequently with obstructive symptoms (n = 54), followed by epistaxis (n = 23), auditory symptoms (n = 12), nerve symptoms (n = 11), nasal discharge (n = 11), and/or visual symptoms (n = 10), present for a mean of 18.2 months. The tumors involved the nasal cavity alone (n = 25), nasopharynx alone (n = 13), maxillary sinus alone (n = 4), or a combination of the nasal cavity and paranasal sinuses (n = 44), with a mean size of 3.7 cm. Patients presented equally between low and high stage disease: stage I and II (n = 42) or stage III and IV (n = 44) disease. Histologically, the tumors were invasive (bone: n = 66; neural: n = 47; lymphovascular: n = 33), composed of a variety of growth patterns, including cribriform (n = 33), tubular (n = 16), and solid (n = 9), although frequently a combination of these patterns was seen within a single tumor. Pleomorphism was mild with an intermediate N:C ratio in cells containing hyperchromatic nuclei. Reduplicated basement membrane and glycosaminoglycan material was commonly seen. Necrosis (n = 16) and atypical mitotic figures (n = 11) were infrequently present. Pleomorphic adenoma was present in 9 cases; de-differentiation was seen in two patients. Immunohistochemical studies showed positive reactions for pan-cytokeratin, CK7, CK5/6, CAM5.2, and EMA, with myoepithelial reactivity with SMA, p63, calponin, S100 protein and SMMHC. CD117, CEA, GFAP and p16 were variably present. CK20 and HR HPV were negative. STACC needs to be considered in the differential diagnosis of most sinonasal malignancies, particularly poorly differentiated carcinoma, olfactory neuroblastoma and pleomorphic adenoma. Surgery (n = 82), often accompanied by radiation therapy (n = 36), was generally employed. A majority of patients developed a recurrence (n = 52) 2-144 months after initial presentation. Overall mean follow-up was 19.4 years (range 0.4-37.5 years): 46 patients died with disease (mean 6.4 years); 5 were alive with disease (mean 5.4 years), and 35 patients were either alive or had died of unrelated causes (mean 16.3 years). ACC of the SNT is uncommon. Recurrences are common. The following parameters, when present, suggest an increased incidence of either recurrence or dying with disease: mixed site of involvement, high stage disease (stage IV), skull base involvement, tumor recurrence, a solid histology, perineural invasion, bone invasion, and lymphovascular invasion.
Figures
References
-
- Eveson JW. Salivary gland-type carcinomas. In: Barnes L, Eveson JW, Reichart P, Sidransky D, editors. Pathology and genetics: head and neck tumours. Lyon: IARC Press; 2005. pp. 24–25.
-
- Franchi A, Santucci M, Wenig BM. Adenocarcinoma. In: Barnes EL, Eveson JW, Reichart P, Sidransky D, editors. Pathology and genetics head and neck tumours. Lyon: IARC Press; 2005. pp. 20–23.
-
- Kleinsasser O, Schroeder HG. Adenocarcinomas of the inner nose after exposure to wood dust. Morphological findings and relationships between histopathology and clinical behavior in 79 cases. Arch Otorhinolaryngol. 1988;245:1–15. - PubMed
-
- Barnes L. Intestinal-type adenocarcinoma of the nasal cavity and paranasal sinuses. Am J Surg Pathol. 1986;10:192–202. - PubMed
-
- Gnepp DR, Heffner DK. Mucosal origin of sinonasal tract adenomatous neoplasms. Mod Pathol. 1989;2:365–371. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
