

Trial of recombinant follicle-stimulating hormone pretreatment for GnRH-induced fertility in patients with congenital hypogonadotropic hypogonadism
- PMID: 24037890
- PMCID: PMC3816270
- DOI: 10.1210/jc.2013-2518
Trial of recombinant follicle-stimulating hormone pretreatment for GnRH-induced fertility in patients with congenital hypogonadotropic hypogonadism
Abstract
Context and objective: The optimal strategy for inducing fertility in men with congenital hypogonadotropic hypogonadism (CHH) is equivocal. Albeit a biologically plausible approach, pretreatment with recombinant FSH (rFSH) before GnRH/human chorionic gonadotropin administration has not been sufficiently assessed. The objective of the study was to test this method.
Design and setting: This was a randomized, open-label treatment protocol at an academic medical center.
Patients and interventions: GnRH-deficient men (CHH) with prepubertal testes (<4 mL), no cryptorchidism, and no prior gonadotropin therapy were randomly assigned to either 24 months of pulsatile GnRH therapy alone (inducing endogenous LH and FSH release) or 4 months of rFSH pretreatment followed by 24 months of GnRH therapy. Patients underwent serial testicular biopsies, ultrasound assessments of testicular volume, serum hormone measurements, and seminal fluid analyses.
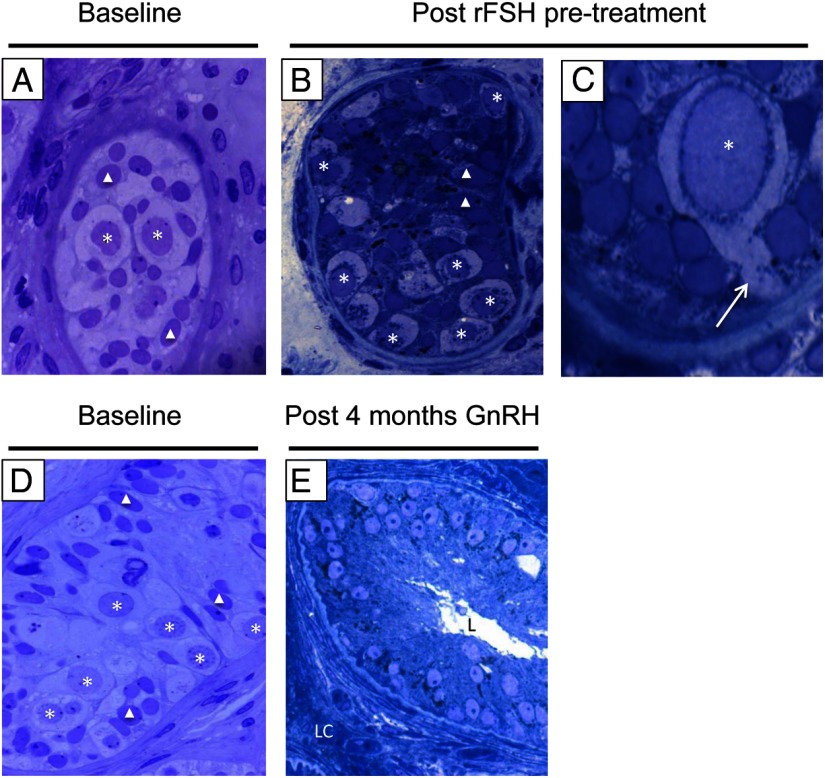
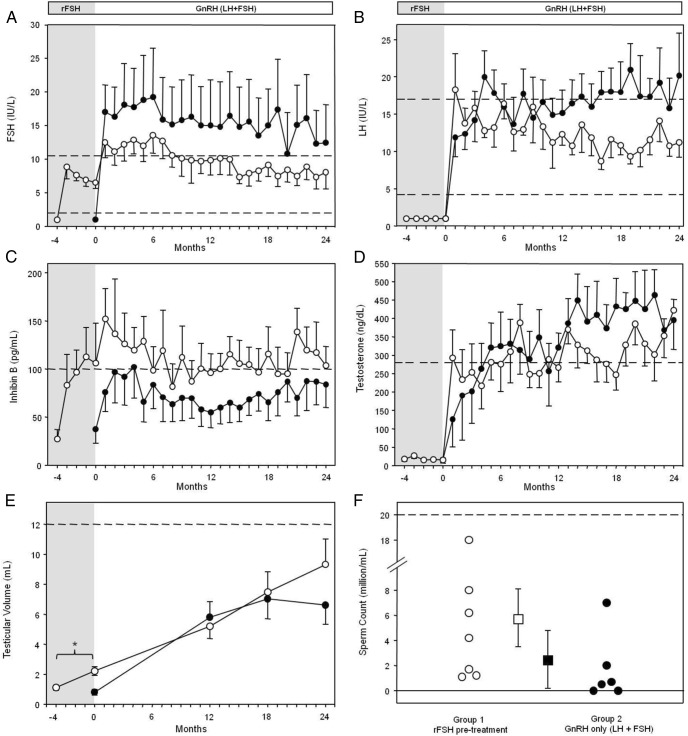
Results: rFSH treatment increased inhibin B levels into the normal range (from 29 ± 9 to 107 ± 41 pg/mL, P < .05) and doubled testicular volume (from 1.1 ± 0.2 to 2.2 ± 0.3 mL, P < .005). Histological analysis showed proliferation of both Sertoli cells (SCs) and spermatogonia, a decreased SC to germ cell ratio (from 0.74 to 0.35), and SC cytoskeletal rearrangements. With pulsatile GnRH, the groups had similar hormonal responses and exhibited significant testicular growth. All men receiving rFSH pretreatment developed sperm in their ejaculate (7 of 7 vs 4 of 6 in the GnRH-only group) and showed trends toward higher maximal sperm counts.
Conclusions: rFSH pretreatment followed by GnRH is successful in inducing testicular growth and fertility in men with CHH with prepubertal testes. rFSH not only appears to maximize the SC population but also induces morphologic changes, suggesting broader developmental roles.
Trial registration: ClinicalTrials.gov NCT00064987.
Figures
References
-
- Cortes D, Müller J, Skakkebaek NE. Proliferation of Sertoli cells during development of the human testis assessed by stereological methods. Int J Androl. 1987;10:589–596 - PubMed
-
- Müller J, Skakkebaek NE. Quantification of germ cells and seminiferous tubules by stereological examination of testicles from 50 boys who suffered from sudden death. Int J Androl. 1983;6:143–156 - PubMed
-
- Regadera J, Martínez-Garcia F, González-Peramato P, Serrano A, Nistal M, Suárez-Quian C. Androgen receptor expression in Sertoli cells as a function of seminiferous tubule maturation in the human cryptorchid testis. J Clin Endocrinol Metab. 2001;86:413–421 - PubMed
-
- Andersson AM, Müller J, Skakkebaek NE. Different roles of prepubertal and postpubertal germ cells and Sertoli cells in the regulation of serum inhibin B levels. J Clin Endocrinol Metab. 1998;83:4451–4458 - PubMed
-
- Orth JM, Gunsalus GL, Lamperti AA. Evidence from Sertoli cell-depleted rats indicates that spermatid number in adults depends on numbers of Sertoli cells produced during perinatal development. Endocrinology. 1988;122:787–794 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
