

Most patients with cancer-associated dermatomyositis have antibodies to nuclear matrix protein NXP-2 or transcription intermediary factor 1γ
- PMID: 24037894
- PMCID: PMC4073292
- DOI: 10.1002/art.38093
Most patients with cancer-associated dermatomyositis have antibodies to nuclear matrix protein NXP-2 or transcription intermediary factor 1γ
Abstract
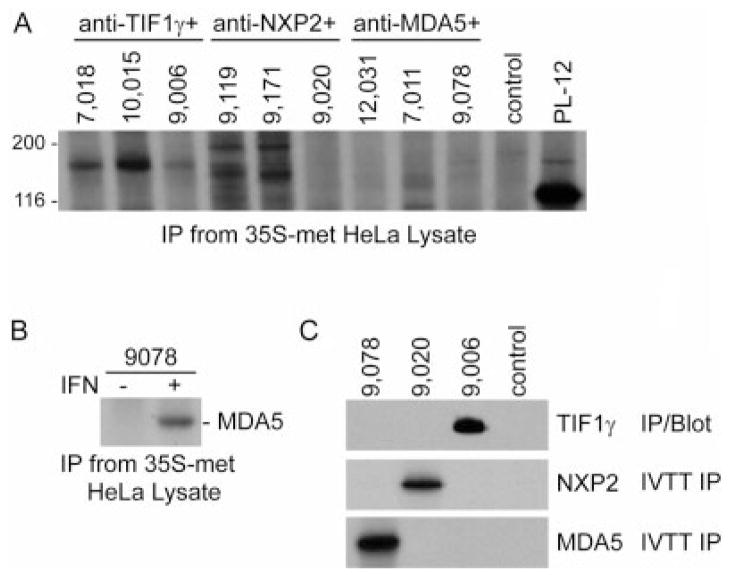
Objective: Since dermatomyositis (DM) is associated with an increased risk of malignancy, accurate identification of patients likely to harbor cancers is important. Using immunoprecipitations from radiolabeled cell lysates, several groups recently showed that anti-transcription intermediary factor 1γ (anti-TIF-1γ) antibodies are associated with malignancy in DM. We undertook this study to develop sensitive, specific assays to detect antibodies against TIF-1γ and nuclear matrix protein NXP-2 and to evaluate their association with malignancy in DM.
Methods: To detect anti-TIF-1γ antibodies, immunoprecipitations were performed using lysates made from HeLa cells overexpressing TIF-1γ, with detection by immunoblotting. Anti-NXP-2 antibodies were assayed by immunoprecipitation using (35) S-methionine-labeled NXP-2 generated by in vitro transcription/translation. We analyzed patient sera from DM cohorts seen at the Stanford University Dermatology Clinic (n = 111) and the Johns Hopkins Myositis Center (n = 102).
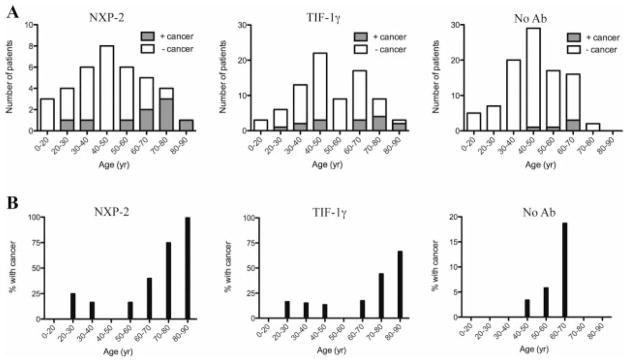
Results: A total of 17% and 38% of patients had antibodies against NXP-2 and TIF-1γ, respectively. Reactivity against either NXP-2 or TIF-1γ identified 83% of patients with cancer-associated DM. In addition to older age and male sex, cancer was associated with antibodies to NXP-2 or TIF-1γ on multivariate analysis (odds ratio 3.78 [95% confidence interval 1.33-10.8]). Stratification by sex revealed that anti-NXP-2 was specifically associated with cancer in males (odds ratio 5.78 [95% confidence interval 1.35-24.7]).
Conclusion: These studies demonstrate that anti-NXP-2 and anti-TIF-1γ antibodies are frequent DM specificities (found in 55% of patients) and are present in most patients with cancer-associated DM.
Copyright © 2013 by the American College of Rheumatology.
Figures
References
-
- Madan V, Chinoy H, Griffiths CE, Cooper RG. Defining cancer risk in dermatomyositis: part I. Clin Exp Dermatol. 2009;34:451–5. - PubMed
-
- Fujimoto M, Hamaguchi Y, Kaji K, Matsushita T, Ichimura Y, Kodera M, et al. Myositis-specific anti-155/140 autoantibodies target transcription intermediary factor 1 family proteins. Arthritis Rheum. 2012;64:513–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
