

Hepatic histological findings in suspected drug-induced liver injury: systematic evaluation and clinical associations
- PMID: 24037963
- PMCID: PMC3946736
- DOI: 10.1002/hep.26709
Hepatic histological findings in suspected drug-induced liver injury: systematic evaluation and clinical associations
Abstract
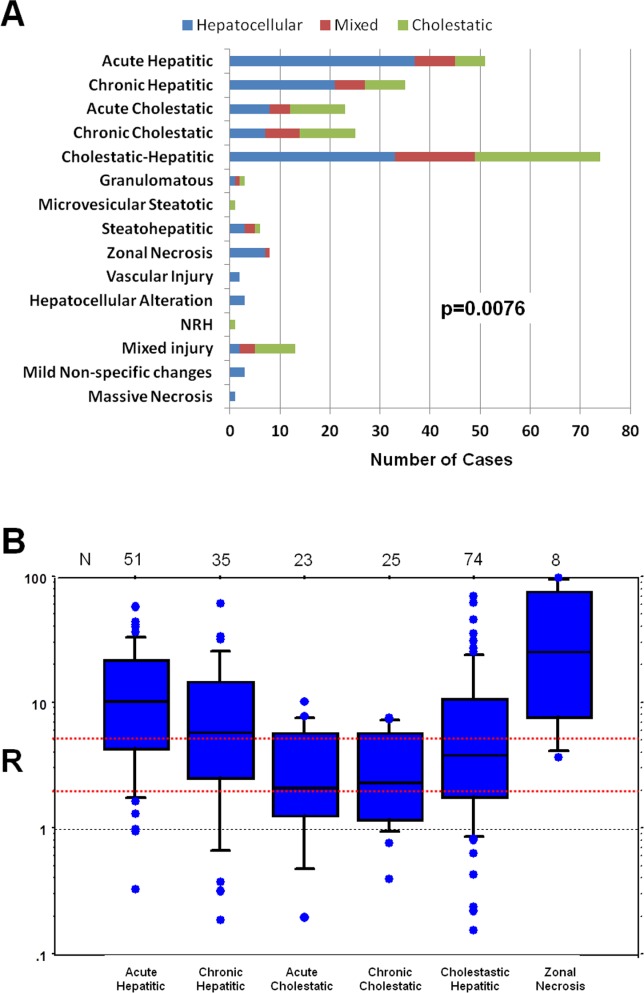
Drug-induced liver injury (DILI) is considered to be a diagnosis of exclusion. Liver biopsy may contribute to diagnostic accuracy, but the histological features of DILI and their relationship to biochemical parameters and outcomes are not well defined. We have classified the pathological pattern of liver injury and systematically evaluated histological changes in liver biopsies obtained from 249 patients with suspected DILI enrolled in the prospective, observational study conducted by the Drug Induced Liver Injury Network. Histological features were analyzed for their frequency within different clinical phenotypes of liver injury and to identify associations between clinical and laboratory findings and histological features. The most common histological patterns were acute (21%) and chronic hepatitis (14%), acute (9%) and chronic cholestasis (10%), and cholestatic hepatitis (29%). Liver histology from 128 patients presenting with hepatocellular injury had more severe inflammation, necrosis, and apoptosis and more frequently demonstrated lobular disarray, rosette formation, and hemorrhage than those with cholestasis. Conversely, histology of the 73 patients with cholestatic injury more often demonstrated bile plugs and duct paucity. Severe or fatal hepatic injury in 46 patients was associated with higher degrees of necrosis, fibrosis stage, microvesicular steatosis, and ductular reaction among other findings, whereas eosinophils and granulomas were found more often in those with milder injury.
Conclusion: We describe an approach for evaluating liver histology in DILI and demonstrate numerous associations between pathological findings and clinical presentations that may serve as a foundation for future studies correlating DILI pathology with its causality and outcome.
Copyright © 2013 The Authors. HEPATOLOGY published by Wiley on behalf of the American Association for the Study of Liver Diseases.
Figures
References
-
- Ostapowicz G, Fontana RJ, Schiodt FV, Larson A, Davern TJ, Han SH. Results of a prospective study of acute liver failure at 17 tertiary care centers in the United States. Ann Intern Med. 2002;137:947–954. et al. - PubMed
-
- Lee WM, Senior JR. Recognizing drug-induced liver injury: current problems, possible solutions. Toxicol Pathol. 2005;33:155–164. - PubMed
-
- Shapiro MA, Lewis JH. Causality assessment of drug-induced hepatotoxicity: promises and pitfalls. Clin Liver Dis. 2007;11:477–505. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DK065211/DK/NIDDK NIH HHS/United States
- U01DK065176/DK/NIDDK NIH HHS/United States
- U01DK065193/DK/NIDDK NIH HHS/United States
- U01DK083020/DK/NIDDK NIH HHS/United States
- U01 DK083027/DK/NIDDK NIH HHS/United States
- U01 DK065201/DK/NIDDK NIH HHS/United States
- U01 DK065238/DK/NIDDK NIH HHS/United States
- U01DK83023/DK/NIDDK NIH HHS/United States
- U01 DK065176/DK/NIDDK NIH HHS/United States
- U01 DK083023/DK/NIDDK NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- U01DK08992/DK/NIDDK NIH HHS/United States
- U01DK065201/DK/NIDDK NIH HHS/United States
- U01 DK082992/DK/NIDDK NIH HHS/United States
- U01 DK083020/DK/NIDDK NIH HHS/United States
- U01DK083027/DK/NIDDK NIH HHS/United States
- U01DK065238/DK/NIDDK NIH HHS/United States
- U01DK065211/DK/NIDDK NIH HHS/United States
- U01DK065184/DK/NIDDK NIH HHS/United States
- U01 DK065184/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical