

Efficacy, safety and survival with ruxolitinib in patients with myelofibrosis: results of a median 2-year follow-up of COMFORT-I
- PMID: 24038026
- PMCID: PMC3856961
- DOI: 10.3324/haematol.2013.092155
Efficacy, safety and survival with ruxolitinib in patients with myelofibrosis: results of a median 2-year follow-up of COMFORT-I
Abstract
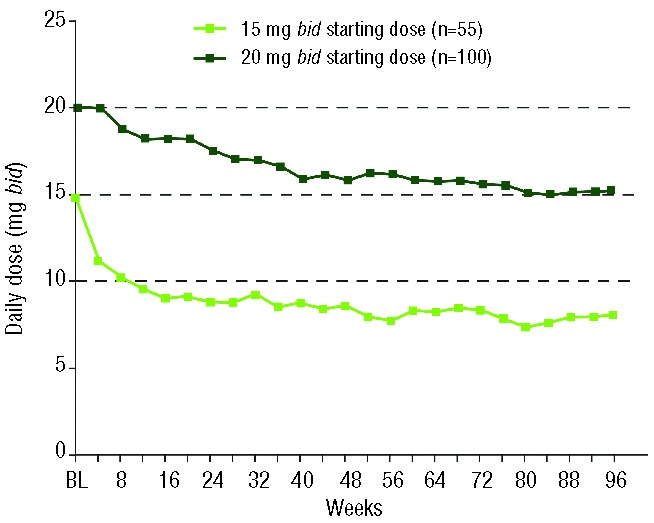
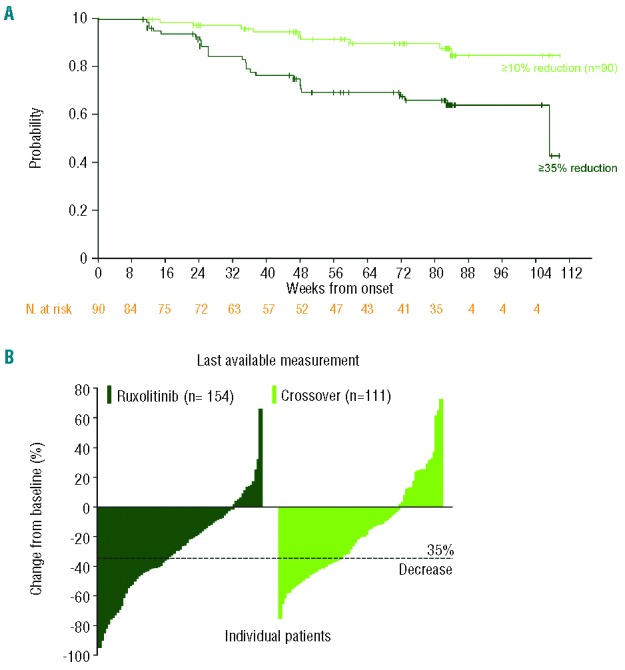
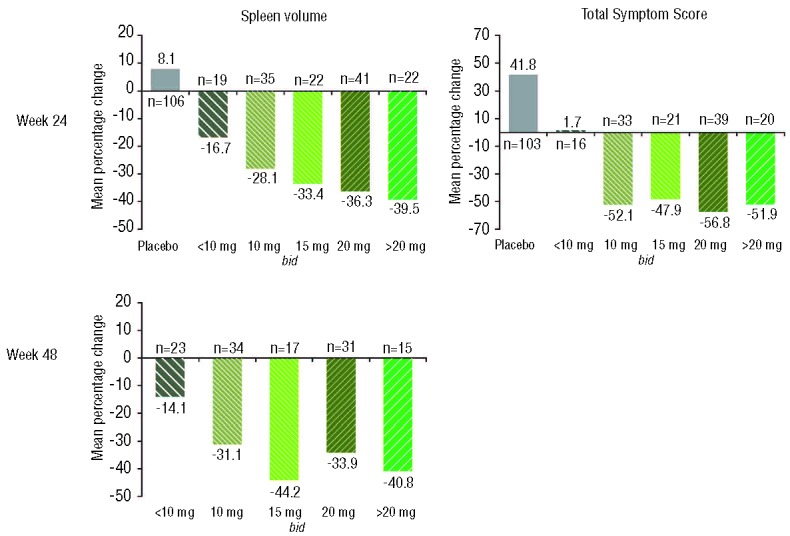
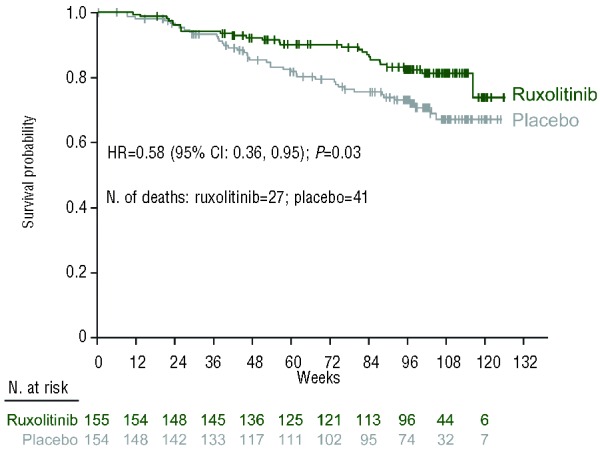
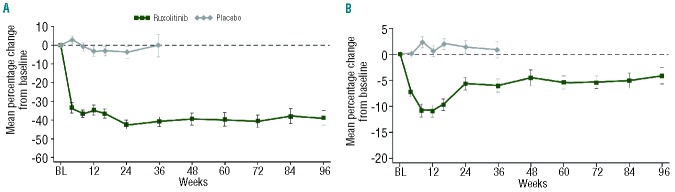
COMFORT-I is a randomized, double-blind, placebo-controlled trial of the Janus kinase 1/Janus kinase 2 inhibitor ruxolitinib in 309 patients with intermediate-2 or high-risk myelofibrosis. This analysis of COMFORT-I describes the long-term efficacy and safety of ruxolitinib (median follow-up, 2 years). Spleen volume was measured by magnetic resonance imaging, and quality of life was evaluated using the EORTC QLQ-C30. Overall survival was determined according to randomized treatment group. At the time of this analysis, 100 of 155 patients randomized to ruxolitinib were still receiving treatment. All patients randomized to placebo crossed over to ruxolitinib or discontinued within 3 months of the primary analysis (median time to crossover, 41 weeks). Mean spleen volume reductions in the ruxolitinib group were 31.6% at week 24 and 34.9% at week 96; improvements in quality of life measures were also maintained. Improved survival was observed for ruxolitinib (n=27 deaths) versus placebo (n=41 deaths) (hazard ratio=0.58; 95% confidence interval: 0.36, 0.95; P=0.03). The incidence of new-onset grade 3 or 4 anemia and thrombocytopenia decreased over time to levels observed in patients receiving placebo. These data indicate that ruxolitinib treatment provides durable reductions in spleen volume and improvements in quality of life and suggest a continued survival advantage for ruxolitinib over placebo.
Figures

References
-
- Tefferi A, Vardiman JW. Classification and diagnosis of myeloproliferative neoplasms: the 2008 World Health Organization criteria and point-of-care diagnostic algorithms. Leukemia. 2008;22(1): 14–22 - PubMed
-
- Vannucchi AM. Management of myelofibrosis. Hematology Am Soc Hematol Educ Program. 2011;2011:222–30 - PubMed
-
- Cervantes F, Dupriez B, Pereira A, Passamonti F, Reilly JT, Morra E, et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for Myelofibrosis Research and Treatment. Blood. 2009;113(13): 2895–901 - PubMed
-
- Mesa RA, Niblack J, Wadleigh M, Verstovsek S, Camoriano J, Barnes S, et al. The burden of fatigue and quality of life in myeloproliferative disorders (MPDs): an international Internet-based survey of 1179 MPD patients. Cancer. 2007;109(1): 68–76 - PubMed
-
- Vannucchi AM, Guglielmelli P, Tefferi A. Advances in understanding and management of myeloproliferative neoplasms. CA Cancer J Clin. 2009;59(3): 171–91 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
