

Risk of severe and refractory postoperative nausea and vomiting in patients undergoing diep flap breast reconstruction
- PMID: 24038427
- PMCID: PMC3991126
- DOI: 10.1002/micr.22155
Risk of severe and refractory postoperative nausea and vomiting in patients undergoing diep flap breast reconstruction
Abstract
Background: Postoperative nausea and vomiting (PONV) are commonly feared after general anesthesia and can impact results. The primary aim of our study was to examine incidence and severity of PONV by investigating complete response, or absence of PONV, to prophylaxis used in patients undergoing DIEP flaps. Our secondary aims were definition of the magnitude of risk, state of the art of interventions, clinical sequelae of PONV, and interaction between these variables, specifically for DIEP patients.
Methods: A retrospective chart review occurred for 29 patients undergoing DIEP flap breast reconstruction from September 2007 to February 2008. We assessed known patient and procedure-specific risks for PONV after DIEPs, prophylactic antiemetic regimens, incidence, and severity of PONV, postoperative antiemetic rescues, and effects of risks and treatments on symptoms.
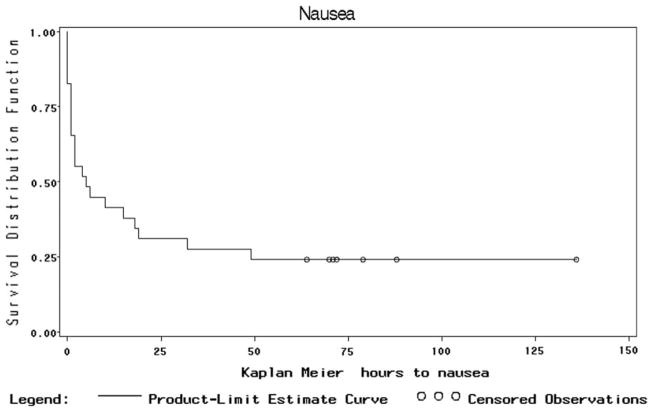
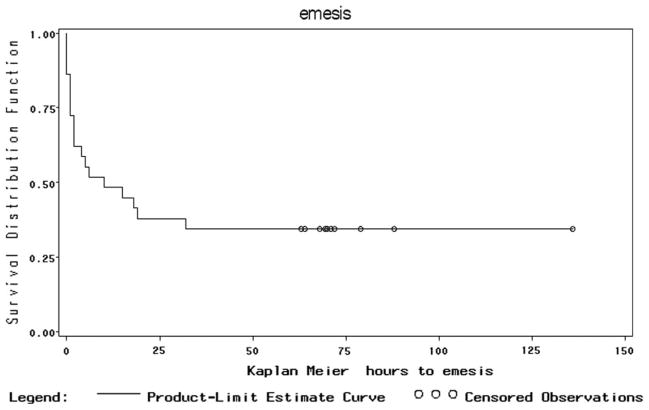
Results: Three or more established risks existed in all patients, with up to seven risks per patient. Although 90% of patients received diverse prophylaxis, 76% of patients experienced PONV, and 66% experienced its severe form, emesis. Early PONV (73%) was frequent; symptoms were long lasting (average 20 hours for nausea and emesis); and multiple rescue medications were frequently required (55% for nausea, 58% for emesis). Length of surgery and nonsmoking statistically significantly impacted PONV.
Conclusion: We identify previously undocumented high risks for PONV in DIEP patients. High frequency, severity, and refractoriness of PONV occur despite standard prophylaxis. Plastic surgeons and anesthesiologists should further investigate methods to optimize PONV prophylaxis and treatment in DIEP flap patients.
© 2013 Wiley Periodicals, Inc.
Figures
References
-
- White PF. Prevention of postoperative nausea and vomiting-a multimodal solution to a persistent problem. NEJM. 2004;350:2511–2512. - PubMed
-
- Kovac AL, Eberhart L, Kotarski J, Clerici G, Apfel C. A randomized, double-blind study to evaluate the efficacy and safety of three different doses of palonosetron versus placebo in preventing postoperative nausea and vomiting over a 72-hour period. Anesth Analg. 2008;107:439–444. - PubMed
-
- Layeeque R, Siegel E, Kass R, Henry-Tillman RS, Colvert M, Mancino A, Klimberg VS. Prevention of nausea and vomiting following breast surgery. Am J Surg. 2006;191:767–772. - PubMed
-
- Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg. 1999;89:652–658. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
