

Postconcussional disorder and PTSD symptoms of military-related traumatic brain injury associated with compromised neurocircuitry
- PMID: 24038816
- PMCID: PMC6869078
- DOI: 10.1002/hbm.22358
Postconcussional disorder and PTSD symptoms of military-related traumatic brain injury associated with compromised neurocircuitry
Abstract
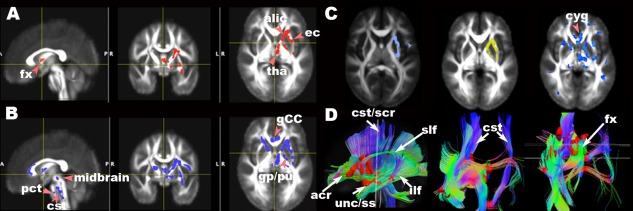
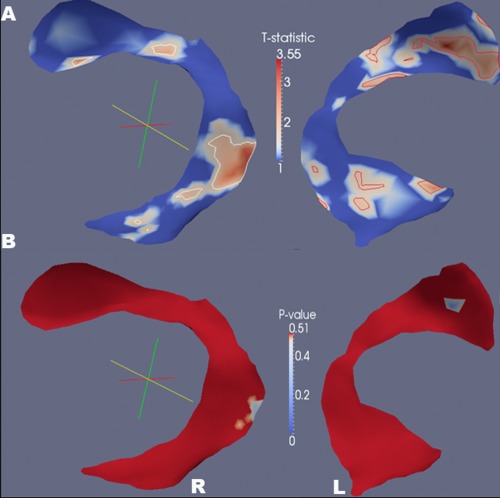
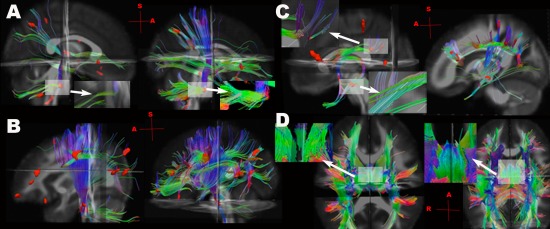
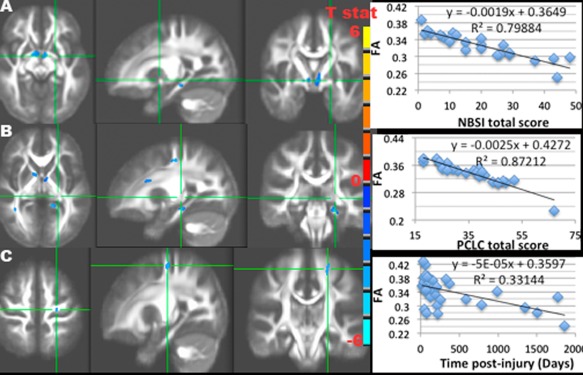
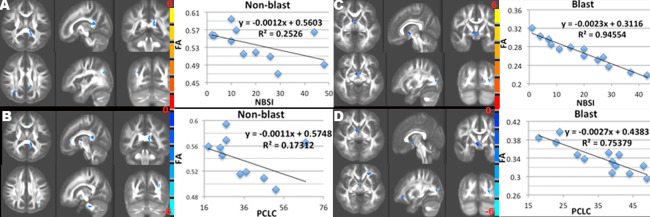
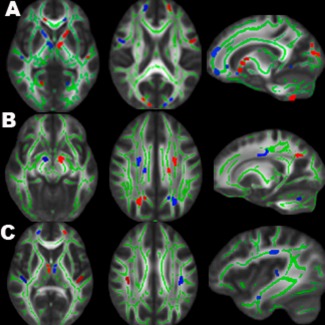
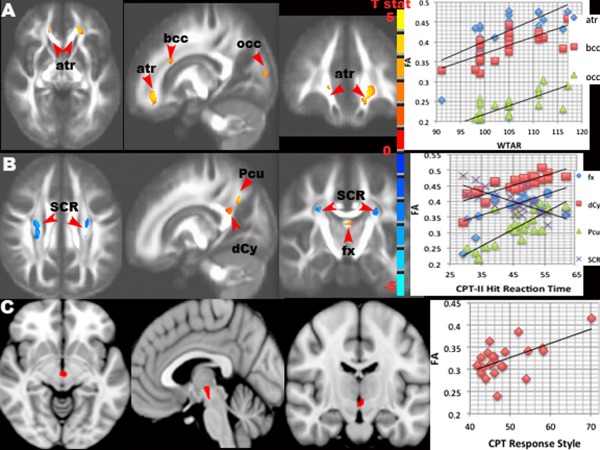
Traumatic brain injury (TBI) is a common combat injury, often through explosive blast, and produces heterogeneous brain changes due to various mechanisms of injury. It is unclear whether the vulnerability of white matter differs between blast and impact injury, and the consequences of microstructural changes on neuropsychological function are poorly understood in military TBI patients. Diffusion tensor imaging (DTI) techniques were used to assess the neurocircuitry in 37 U.S. service members (29 mild, 7 moderate, 1 severe; 17 blast and 20 nonblast), who sustained a TBI while deployed, compared to 14 nondeployed, military controls. High-dimensional deformable registration of MRI diffusion tensor data was followed by fiber tracking and tract-specific analysis along with region-of-interest analysis. DTI results were examined in relation to post-concussion and post-traumatic stress disorder (PTSD) symptoms. The most prominent white matter microstructural injury for both blast and nonblast patients was in the frontal fibers within the fronto-striatal (corona radiata, internal capsule) and fronto-limbic circuits (fornix, cingulum), the fronto-parieto-occipital association fibers, in brainstem fibers, and in callosal fibers. Subcortical superior-inferiorly oriented tracts were more vulnerable to blast injury than nonblast injury, while direct impact force had more detrimental effects on anterior-posteriorly oriented tracts, which tended to cause heterogeneous left and right hemispheric asymmetries of white matter connectivity. The tractography using diffusion anisotropy deficits revealed the cortico-striatal-thalamic-cerebellar-cortical (CSTCC) networks, where increased post-concussion and PTSD symptoms were associated with low fractional anisotropy in the major nodes of compromised CSTCC neurocircuitry, and the consequences on cognitive function were explored as well.
Keywords: blast injury; concussion; diffusion tensor imaging; neurocircuitry; post-traumatic stress disorder; traumatic brain injury.
Copyright © 2013 Wiley Periodicals, Inc.
Figures
References
-
- Adams JH, Doyle D, Ford I, Gennarelli TA, Graham DI, McLellan DR (1989): Diffuse axonal injury in head injury: Definition, diagnosis and grading. Histopathology 15:49–59. - PubMed
-
- Alexander GE, DeLong MR, Strick PL (1986): Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annu Rev Neurosci 9:357–381. - PubMed
-
- Andersson JLR, Jenkinson M, Smith S (2007): Non‐linear optimisation, FMRIB technical report TR07JA1. Oxford, United Kingdom: FMRIB Centre.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
