

Comparative effectiveness of dynamic treatment regimes: an application of the parametric g-formula
- PMID: 24039638
- PMCID: PMC3769803
- DOI: 10.1007/s12561-011-9040-7
Comparative effectiveness of dynamic treatment regimes: an application of the parametric g-formula
Abstract
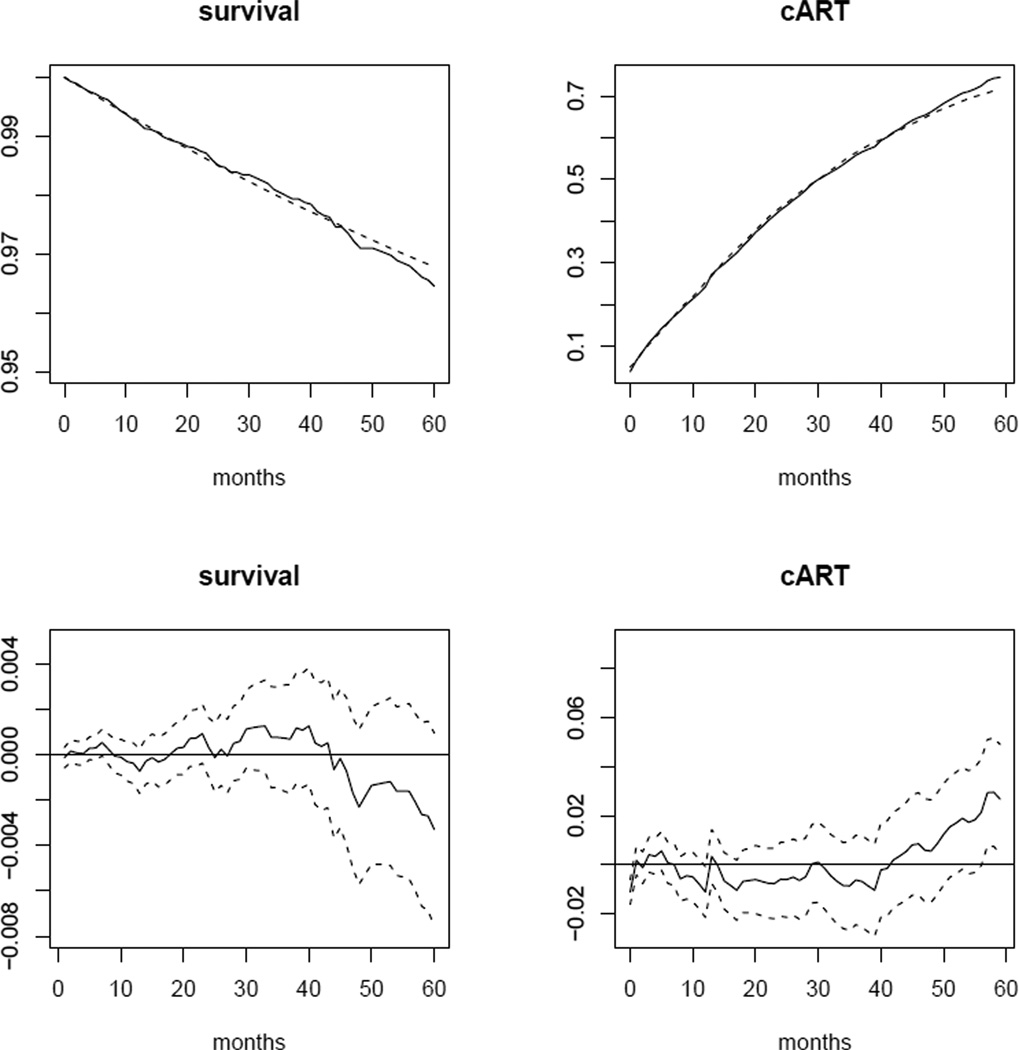
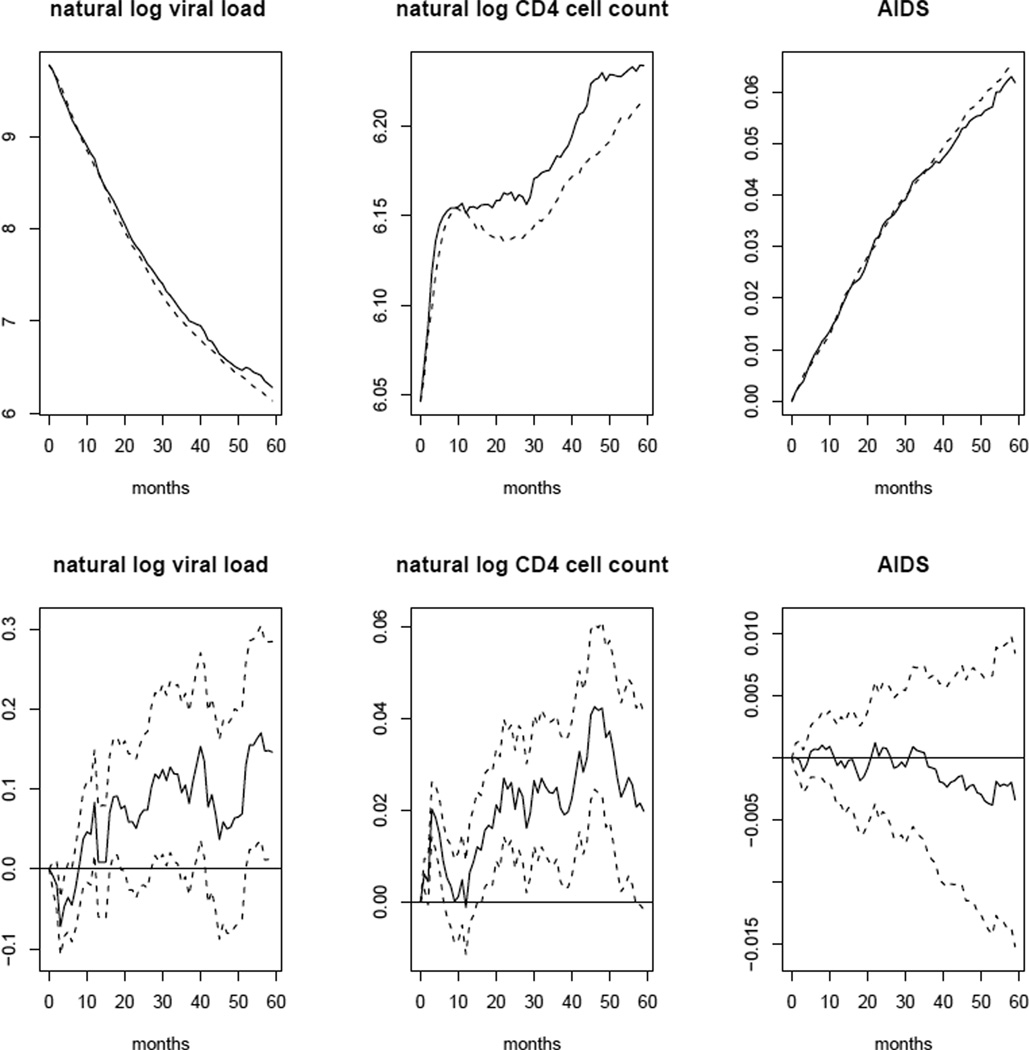
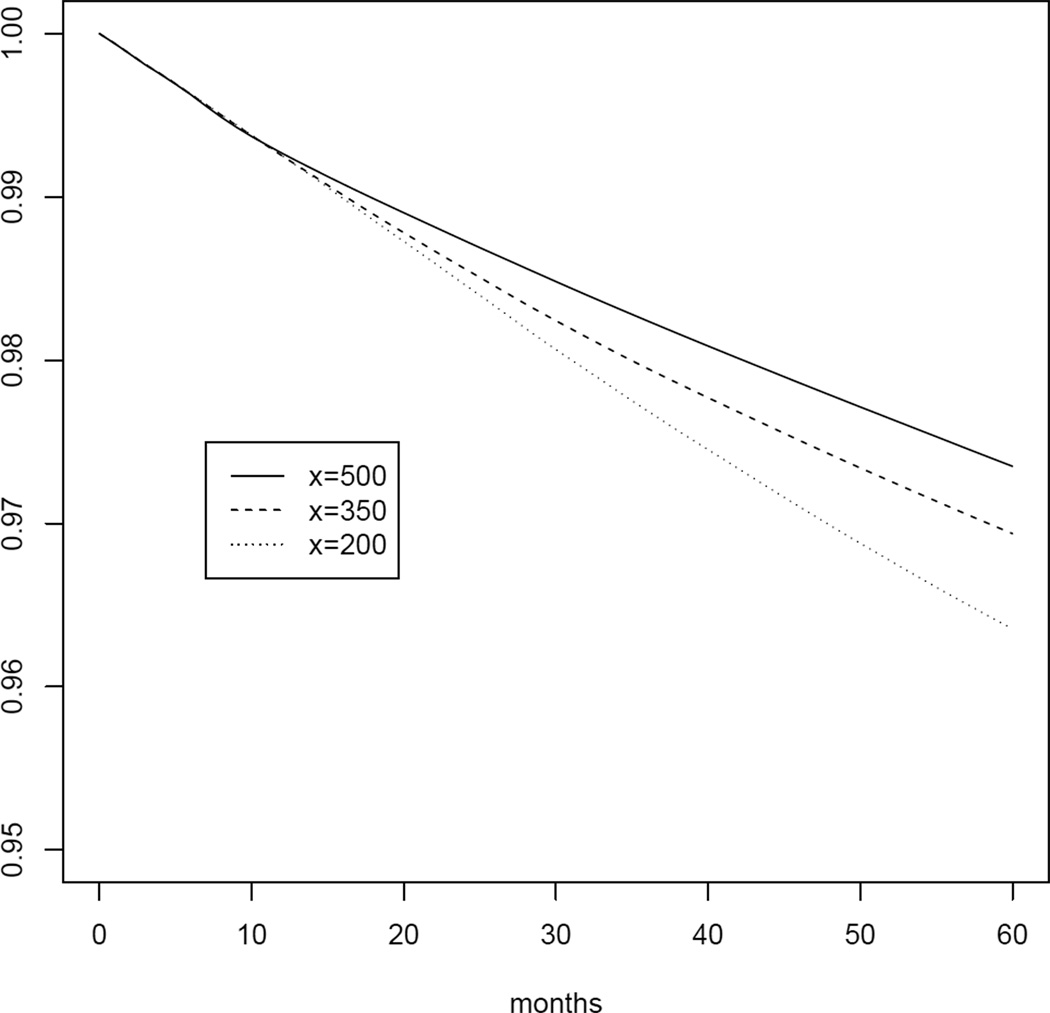
Ideally, randomized trials would be used to compare the long-term effectiveness of dynamic treatment regimes on clinically relevant outcomes. However, because randomized trials are not always feasible or timely, we often must rely on observational data to compare dynamic treatment regimes. An example of a dynamic treatment regime is "start combined antiretroviral therapy (cART) within 6 months of CD4 cell count first dropping below x cells/mm3 or diagnosis of an AIDS-defining illness, whichever happens first" where x can take values between 200 and 500. Recently, Cain et al (2011) used inverse probability (IP) weighting of dynamic marginal structural models to find the x that minimizes 5-year mortality risk under similar dynamic regimes using observational data. Unlike standard methods, IP weighting can appropriately adjust for measured time-varying confounders (e.g., CD4 cell count, viral load) that are affected by prior treatment. Here we describe an alternative method to IP weighting for comparing the effectiveness of dynamic cART regimes: the parametric g-formula. The parametric g-formula naturally handles dynamic regimes and, like IP weighting, can appropriately adjust for measured time-varying confounders. However, estimators based on the parametric g-formula are more efficient than IP weighted estimators. This is often at the expense of more parametric assumptions. Here we describe how to use the parametric g-formula to estimate risk by the end of a user-specified follow-up period under dynamic treatment regimes. We describe an application of this method to answer the "when to start" question using data from the HIV-CAUSAL Collaboration.
Figures
References
-
- Bang H, Robins JM. Doubly robust estimation in missing data and causal inference models. Biometrics. 2005;61:692–972. - PubMed
-
- Cain LE, Logan R, Robins JM, Sterne JA, Sabin C, Bansi L, Justice A, Goulet J, van Sighem A, de Wolf F, Bucher HC, von Wyl V, Esteve A, Casabona J, del Amo J, Moreno S, Meyer L, Pérez-Hoyos S, Muga R, Lodi S, Lanoy E, Costagliola D, Hernán MA on behalf of The HIV-CAUSAL Collaboration. When to initiate combined antiretroviral therapy to reduce rates of mortality and AIDS in HIV-infected individuals in developed countries. Annals of Internal Medicine. 2011;154(8):509–515. - PMC - PubMed
-
- Cameron DW, Heath-Chiozzi M, Danner S, Cohen C, Kravcik S, Maurath C, Sun E, Henry D, Rode R, Potthoff A, Leonard J. Randomised placebo-controlled trial of ritonavir in advanced HIV-1 disease. The Advanced HIV Disease Ritonavir Study Group. The Lancet. 1998;351(9102):543–549. - PubMed
-
- CDC. 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR. 1992;41:1–19. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials