

Clinical predictors and accuracy of empiric tuberculosis treatment among sputum smear-negative HIV-infected adult TB suspects in Uganda
- PMID: 24040151
- PMCID: PMC3765314
- DOI: 10.1371/journal.pone.0074023
Clinical predictors and accuracy of empiric tuberculosis treatment among sputum smear-negative HIV-infected adult TB suspects in Uganda
Abstract
Introduction: The existing diagnostic algorithms for sputum smear-negative tuberculosis (TB) are complicated, time-consuming, and often difficult to implement. The decision to initiate TB treatment in resource-limited countries is often largely based on clinical predictors. We sought to determine the clinical predictors and accuracy of empiric TB treatment initiation in HIV-infected sputum smear-negative TB suspects using sputum culture as a reference standard.
Setting: Out-patient HIV-TB integrated urban clinic in Kampala, Uganda.
Methods: HIV-infected TB suspects were screened using sputum smear microscopy, and mycobacterial sputum liquid and solid cultures were performed. Smear results were made available to the clinician who made a clinical decision on empiric TB treatment initiation for sputum smear-negative patients. Clinic records were reviewed for patients whose sputum smears were negative to collect data on socio-demographics, TB symptomatology, chest X-ray findings, CD4 cell counts and TB treatment initiation.
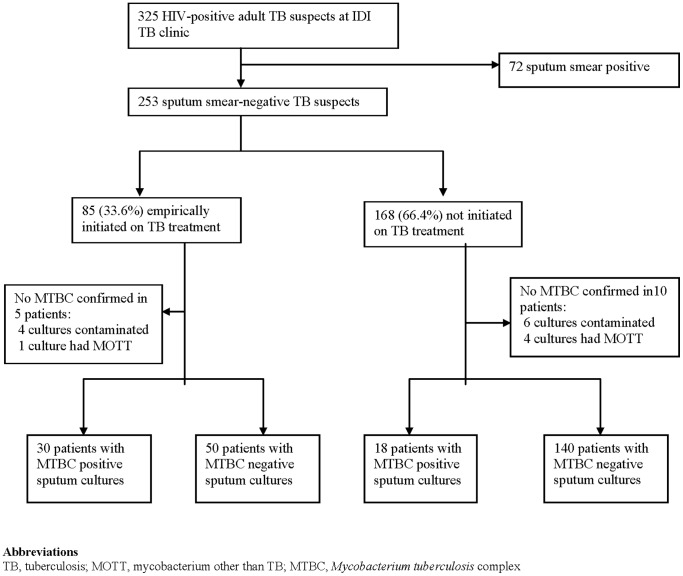
Results: Of 253 smear-negative TB suspects, 56% (142/253) were females, median age 38 IQR (31-44) years, with a median CD4 cell count of 291 IQR (150-482) cells/mm(3). Of the 85 (33.6%) smear-negative patients empirically initiated on TB treatment, 35.3% (n = 30) were sputum culture positive compared to only 18 (10.7%) of the 168 untreated patients (p<0.001). Abnormal chest X-ray [aOR 10.18, 95% CI (3.14-33.00), p<0.001] and advanced HIV clinical stage [aOR 3.92, 95% CI (1.20-12.85), p = 0.024] were significantly associated with empiric TB treatment initiation. The sensitivity and specificity of empiric TB treatment initiation in the diagnosis of TB in HIV-infected patients after negative smear microscopy was 62.5% and 73.7% respectively.
Conclusion: In resource-limited settings, clinically advanced HIV and abnormal chest X-ray significantly predict a clinical decision to empirically initiate TB treatment in smear-negative HIV-infected patients. Empiric TB treatment initiation correlates poorly with TB cultures. Affordable, accurate and rapid point-of-care diagnostics are needed in resource-limited settings to more accurately determine which HIV-infected TB suspects have smear-negative TB.
Conflict of interest statement
Figures
References
-
- Harries AD, Hargreaves NJ, Kemp J, Jindani A, Enarson DA, et al. (2001) Deaths from tuberculosis in sub-Saharan African countries with a high prevalence of HIV-1. Lancet 357: 1519–1523. - PubMed
-
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, et al. (2003) The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med 163: 1009–1021. - PubMed
-
- Elliott AM, Halwiindi B, Hayes RJ, Luo N, Mwinga AG, et al. (1995) The impact of human immunodeficiency virus on mortality of patients treated for tuberculosis in a cohort study in Zambia. Trans R Soc Trop Med Hyg 89: 78–82. - PubMed
-
- Kang’ombe C, Harries AD, Banda H, Nyangulu DS, Whitty CJ, et al. (2000) High mortality rates in tuberculosis patients in Zomba Hospital, Malawi, during 32 months of follow-up. Trans R Soc Trop Med Hyg 94: 305–309. - PubMed
-
- Frieden TR, Sterling TR, Munsiff SS, Watt CJ, Dye C (2003) Tuberculosis. Lancet 362: 887–899. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
