

Uniportal video-assisted thoracoscopic lobectomy
- PMID: 24040531
- PMCID: PMC3771611
- DOI: 10.3978/j.issn.2072-1439.2013.07.30
Uniportal video-assisted thoracoscopic lobectomy
Abstract
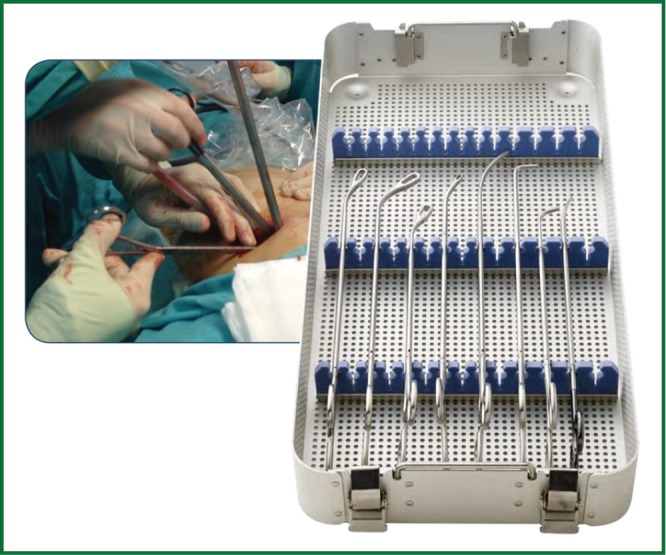
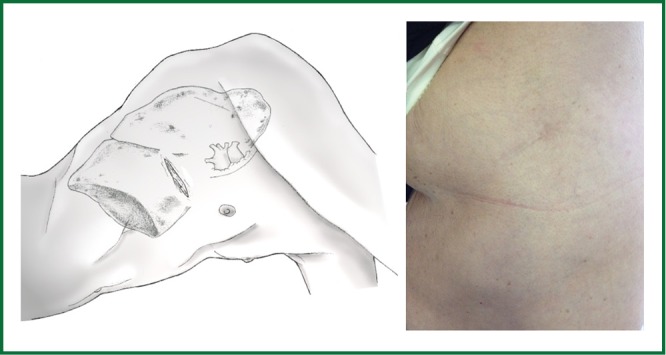
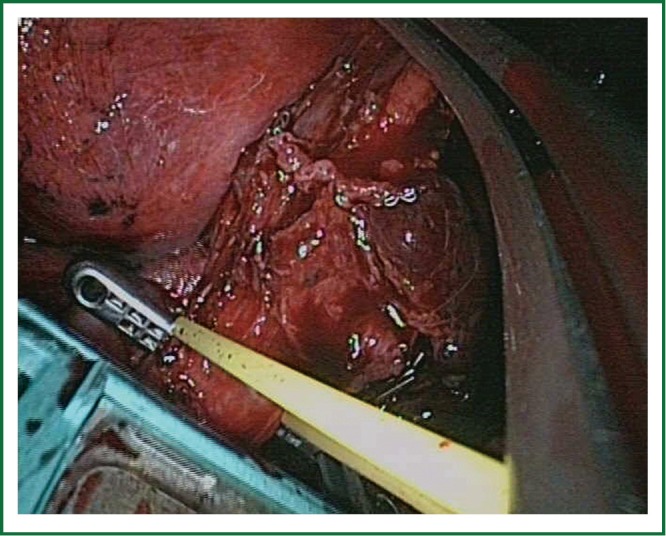
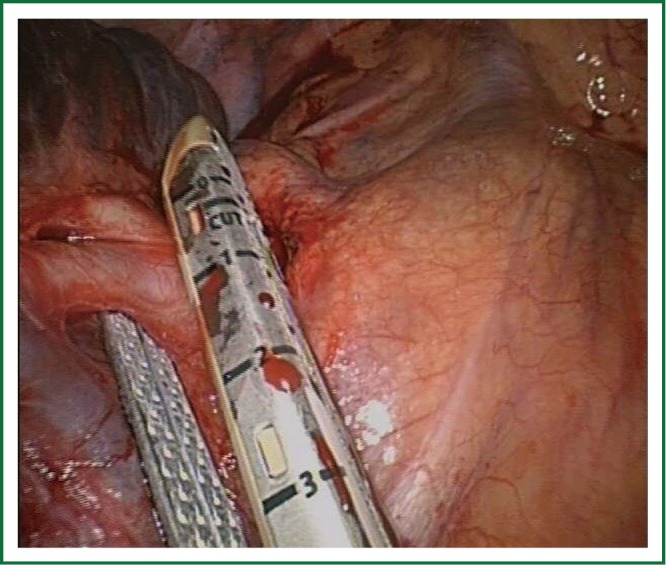
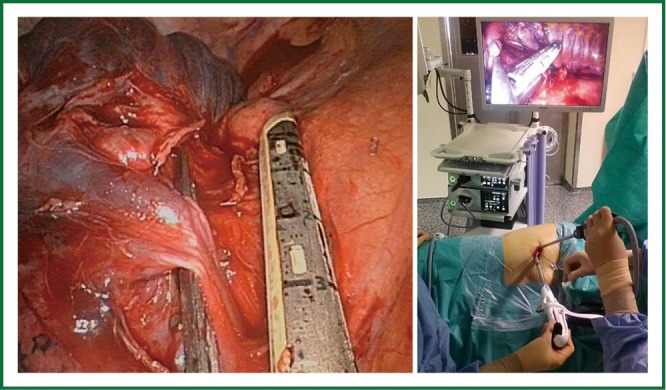
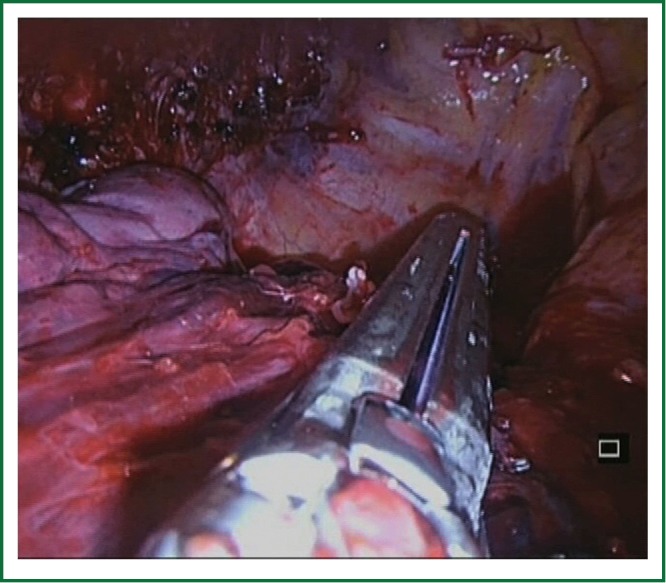
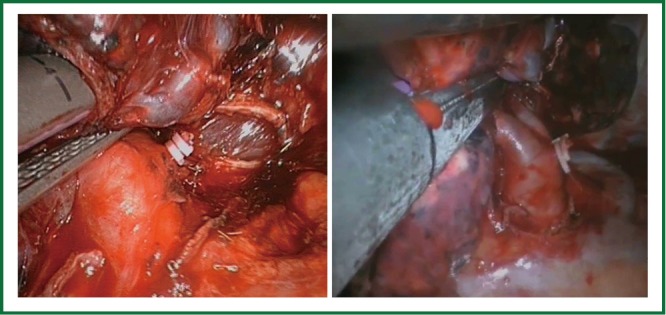
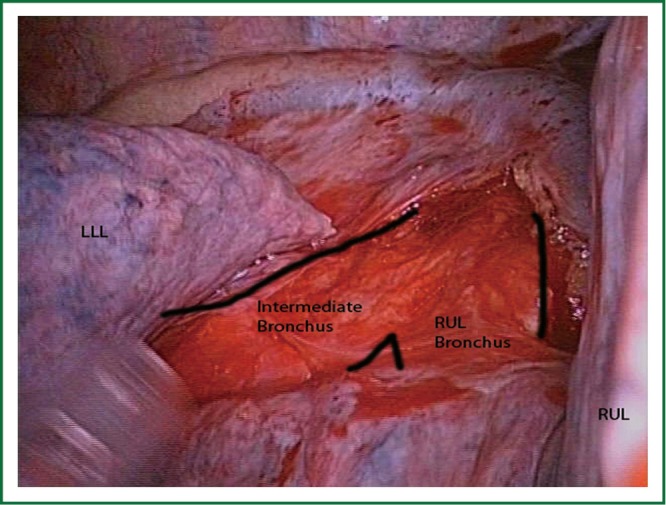
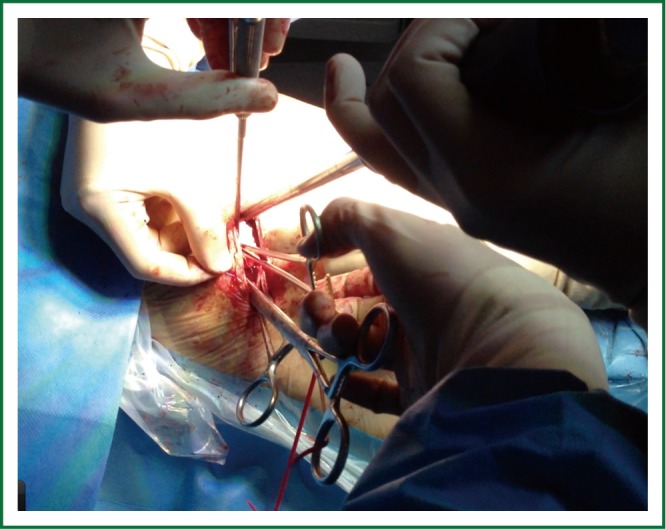
Over the past two decades, video-assisted thoracic surgery (VATS) has revolutionized the way thoracic surgeons diagnose and treat lung diseases. The major advance in VATS procedures is related to the major pulmonary resections. The best VATS technique for lobectomy has not been well defined yet. Most of the authors describe the VATS approach to lobectomy via 3 to 4 incisions but the surgery can be performed by only one incision with similar outcomes. This single incision is the same as we normally use for VATS lobectomies performed by double or triple port technique with no rib spreading. As our experience with VATS lobectomy has grown, we have gradually improved the technique for a less invasive approach. Consequently the greater the experience we gained, the more complex the cases we performed were, hence expanding the indications for single-incision thoracoscopic lobectomy.
Keywords: Video-assisted thoracic surgery (VATS); left lower lobectomy; left upper lobectomy; less invasive approach; lobectomies; lymphadenectomy; middle lobectomy; right lower lobectomy; right upper lobectomy.
Figures






References
-
- Roviaro G, Rebuffat C, Varoli F, et al. Videoendoscopic pulmonary lobectomy for cancer. Surg Laparosc Endosc 1992;2:244-7 - PubMed
-
- Rocco G, Internullo E, Cassivi SD, et al. The variability of practice in minimally invasive thoracic surgery for pulmonary resections. Thorac Surg Clin 2008;18:235-47 - PubMed
-
- Rocco G, Martin-Ucar A, Passera E.Uniportal VATS wedge pulmonary resections. Ann Thorac Surg 2004;77:726-8 - PubMed
-
- Gonzalez D, Paradela M, Garcia J, et al. Single-port video-assisted thoracoscopic lobectomy. Interact Cardiovasc Thorac Surg 2011;12:514-5 - PubMed
-
- McKenna RJ Jr, Mahtabifard A, Swanson SJ. eds. Atlas of minimally invasive thoracic surgery. Saunders 2011;63-5.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous