

An adaptive approach for identifying cocaine dependent patients who benefit from extended continuing care
- PMID: 24041231
- PMCID: PMC3938091
- DOI: 10.1037/a0034265
An adaptive approach for identifying cocaine dependent patients who benefit from extended continuing care
Abstract
Objective: Study tested whether cocaine dependent patients using cocaine or alcohol at intake or in the first few weeks of intensive outpatient treatment would benefit more from extended continuing care than patients abstinent during this period. The effect of incentives for continuing care attendance was also examined.
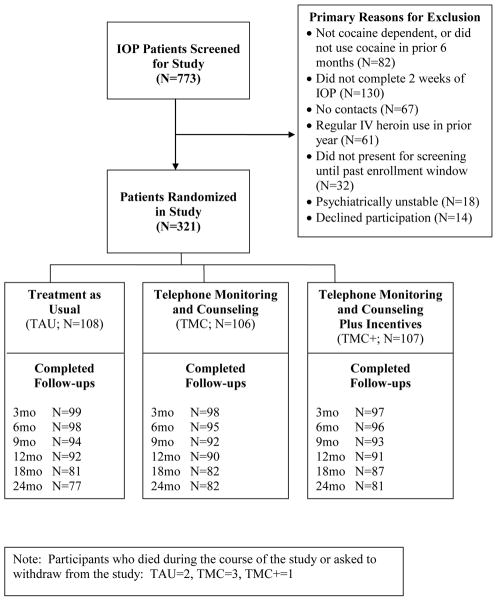
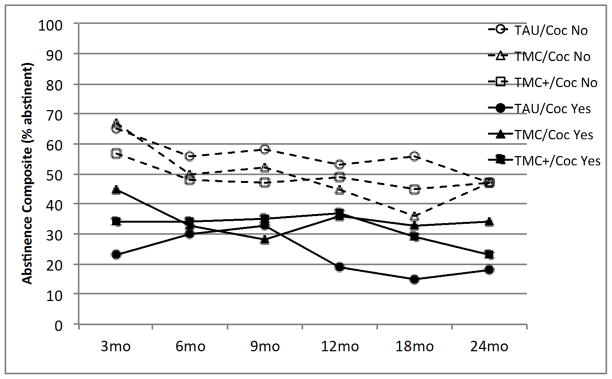
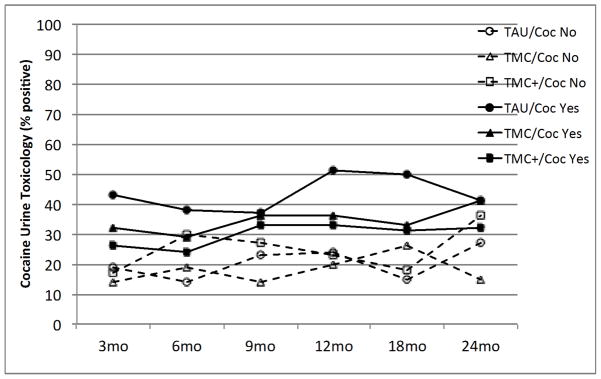
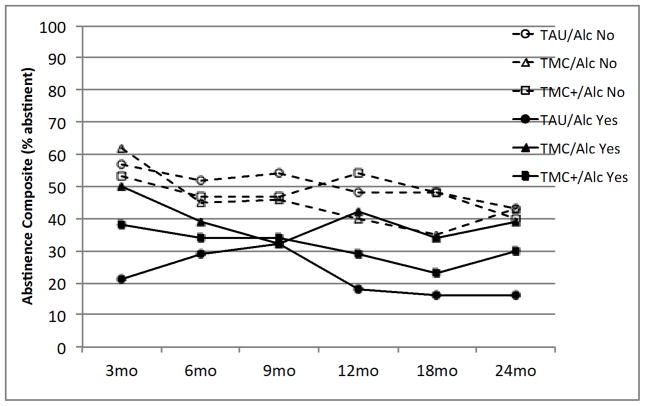
Method: Participants (N = 321) were randomized to treatment as usual (TAU), TAU and telephone monitoring and counseling (TMC), or TAU and TMC plus incentives (TMC+). The primary outcomes were (a) abstinence from all drugs and heavy alcohol use and (b) cocaine urine toxicology. Follow-ups were at 3, 6, 9, 12, 18, and 24 months.
Results: Cocaine and alcohol use at intake or early in treatment predicted worse outcomes on both measures (ps ≤ .0002). Significant effects favoring TMC over TAU on the abstinence composite were obtained in participants who used cocaine (odds ratio [OR] = 1.95 [1.02, 3.73]) or alcohol (OR = 2.47 [1.28, 4.78]) at intake or early in treatment. A significant effect favoring TMC+ over TAU on cocaine urine toxicology was obtained in those using cocaine during that period (OR = 0.55 [0.31, 0.95]). Conversely, there were no treatment effects in participants abstinent at baseline and no overall treatment main effects. Incentives almost doubled the number of continuing care sessions received but did not further improve outcomes.
Conclusion: An adaptive approach for cocaine dependence in which extended continuing care is provided only to patients who are using cocaine or alcohol at intake or early in treatment improves outcomes in this group while reducing burden and costs in lower risk patients.
Figures
References
-
- Alterman AI, Kampman K, Boardman CR, Cacciola JS, Rutherford MJ, McKay JR, Maany IA. Cocaine-positive baseline urine predicts outpatient treatment attrition and failure to attain initial abstinence. Drug and Alcohol Dependence. 1997;46:79–85. - PubMed
-
- Angarita GA, Reif S, Pirad S, Lee S, Sharon E, Gastfriend DR. No-show for treatment in substance abuse patients with comorbid symptomatology: Validity results from a controlled trial of the ASAM Patient Placement Criteria. Journal of Addiction Medicine. 2007;1:79–87. - PubMed
-
- Bride BE, Humble MN. Increasing retention of African-American women on welfare in outpatient substance user treatment using low-magnitude incentives. Substance Use and Misuse. 2008;43:1016–1026. - PubMed
-
- Businelle MS, Rash CJ, Burke RS, Parker JD. Using vouchers to increase continuing care participation in veterans: Does magnitude matter? American Journal of Addiction. 2009;18:122–129. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
