

Lifetime cost-effectiveness of trial of labor after cesarean in the United States
- PMID: 24041345
- PMCID: PMC3983690
- DOI: 10.1016/j.jval.2013.06.014
Lifetime cost-effectiveness of trial of labor after cesarean in the United States
Abstract
Objective: To estimate the cost-effectiveness of a trial of labor after one previous cesarean (TOLAC) when incorporating long-term events and outcomes.
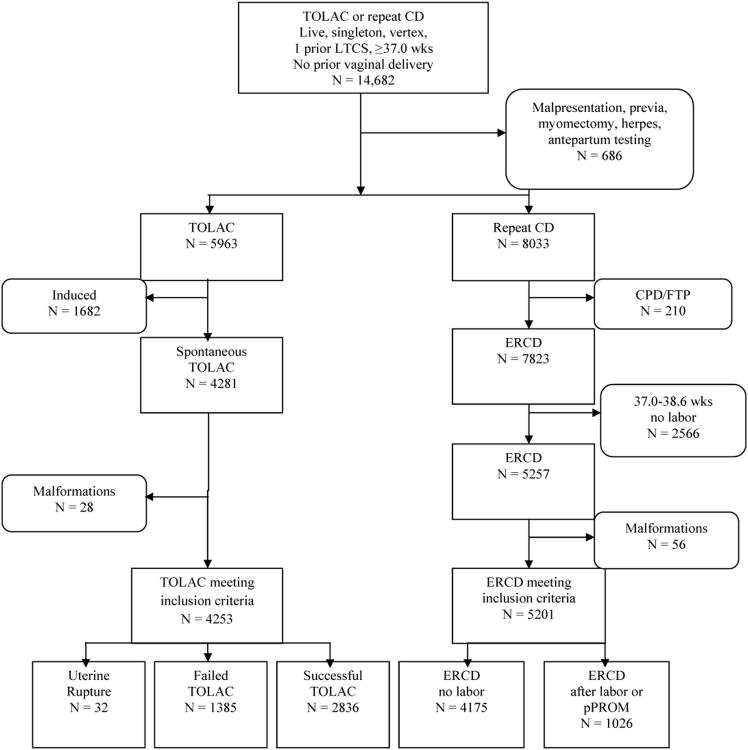
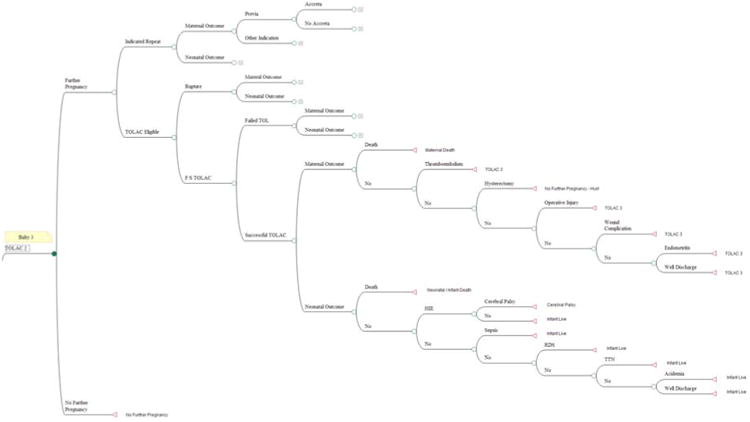
Methods: A Markov model comparing TOLAC with elective repeat cesarean delivery (ERCD) was developed for a hypothetical cohort with no contraindication to a TOLAC. Women were selected from a prospective study to derive probability estimates for potential events through three subsequent pregnancies. Probabilities for cerebral palsy and stress urinary incontinence, cost data, and quality-adjusted life-years (QALYs) were obtained from the literature. The primary outcome was cost-effectiveness measured as the marginal cost per QALY gained, with a $50,000 threshold per QALY used to define cost-effectiveness.
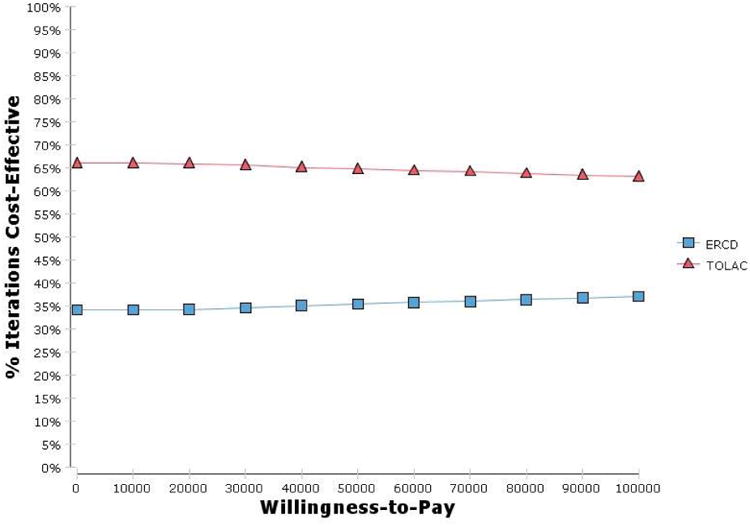
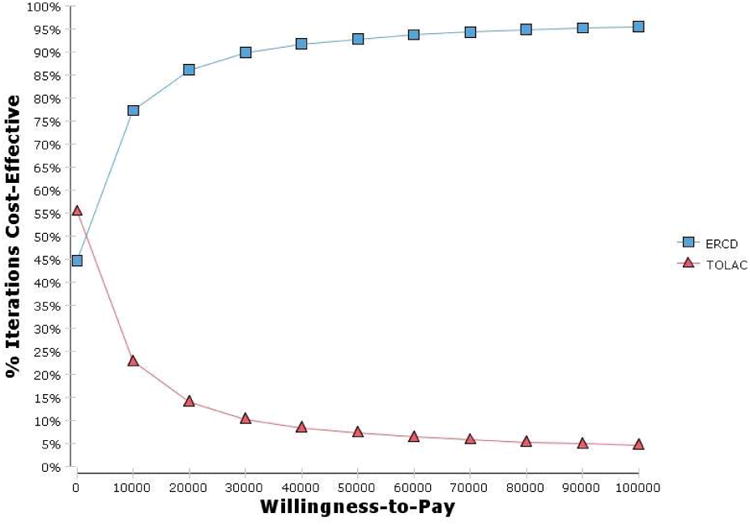
Results: The TOLAC strategy dominated the ERCD strategy at baseline, with $164.2 million saved and 500 QALYs gained per 100,000 women. The model was sensitive to six variables: the probability of uterine rupture and successful TOLAC among women with no prior vaginal delivery, the frequency of stress urinary incontinence, and the costs of failed TOLAC, successful TOLAC, and ERCD. When the probability of TOLAC success was at the base value, 67.2%, TOLAC was preferred if the probability of uterine rupture was 3.1% or less. When the probability of uterine rupture was at the base value, 0.8%, the TOLAC strategy was preferred as long as the probability of success was 47.2% or more. Probabilistic sensitivity analysis confirmed the base-case analysis.
Conclusions: Under baseline circumstances, TOLAC is less expensive and more effective than an ERCD when considering long-term consequences when the likelihood of success is 47.2% or more.
Keywords: accreta; cost-effectiveness; elective repeat; trial of labor.
Copyright © 2013, International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Published by Elsevier Inc.
Conflict of interest statement
None of the authors have a conflict of interest.
Figures
References
-
- MacDorman M, Declerq E, Menacker F. Recent trends and patterns in cesarean birth after cesarean (VBAC) deliveries in the United States. ClinPerinatol. 2011;38:179–92. - PubMed
-
- Martin JA, Hamilton BE, Ventura SJ, et al. National vital statistics reports. 60 no1. Hyattsville, MD: National Center for Health Statistics; 2011. Births: Final data for 2009. - PubMed
-
- Guise JM, Eden K, Emeis C, et al. Evidence/report technology assessment no 191. Rockville, MD: Agency for Healthcare Research and Quality; Mar, 2010. Vaginal birth after cesarean: new insights. Prepared by the Oregon Health & Science University Evidence-based Practice Center under contract no. 290-2007-10057-I. AHRQ publication no. 10-E003.
-
- Chung A, Macario A, El-Sayed YY, et al. Cost-effectiveness of a trial of labor after previous cesarean. Obstet Gynecol. 2001;97:932–41. - PubMed
Publication types
MeSH terms
Grants and funding
- HD36801/HD/NICHD NIH HHS/United States
- UG1 HD027869/HD/NICHD NIH HHS/United States
- U10 HD040544/HD/NICHD NIH HHS/United States
- U10 HD034136/HD/NICHD NIH HHS/United States
- U10 HD040485/HD/NICHD NIH HHS/United States
- HD40485/HD/NICHD NIH HHS/United States
- HD40560/HD/NICHD NIH HHS/United States
- U10 HD040560/HD/NICHD NIH HHS/United States
- U10 HD040512/HD/NICHD NIH HHS/United States
- U01 HD036801/HD/NICHD NIH HHS/United States
- U10 HD040500/HD/NICHD NIH HHS/United States
- HD27861/HD/NICHD NIH HHS/United States
- UG1 HD034116/HD/NICHD NIH HHS/United States
- HD27869/HD/NICHD NIH HHS/United States
- HD34136/HD/NICHD NIH HHS/United States
- UG1 HD040560/HD/NICHD NIH HHS/United States
- HD27860/HD/NICHD NIH HHS/United States
- UG1 HD027915/HD/NICHD NIH HHS/United States
- HD21414/HD/NICHD NIH HHS/United States
- U10 HD027905/HD/NICHD NIH HHS/United States
- HD40512/HD/NICHD NIH HHS/United States
- UG1 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD034208/HD/NICHD NIH HHS/United States
- UG1 HD040512/HD/NICHD NIH HHS/United States
- HD40545/HD/NICHD NIH HHS/United States
- U10 HD034116/HD/NICHD NIH HHS/United States
- HD34210/HD/NICHD NIH HHS/United States
- HD21410/HD/NICHD NIH HHS/United States
- U10 HD027869/HD/NICHD NIH HHS/United States
- U10 HD027917/HD/NICHD NIH HHS/United States
- HD34116/HD/NICHD NIH HHS/United States
- U10 HD034122/HD/NICHD NIH HHS/United States
- U10 HD027915/HD/NICHD NIH HHS/United States
- UG1 HD040545/HD/NICHD NIH HHS/United States
- UG1 HD040485/HD/NICHD NIH HHS/United States
- U10 HD027860/HD/NICHD NIH HHS/United States
- HD40500/HD/NICHD NIH HHS/United States
- U10 HD034208/HD/NICHD NIH HHS/United States
- HD34208/HD/NICHD NIH HHS/United States
- HD27915/HD/NICHD NIH HHS/United States
- UG1 HD040500/HD/NICHD NIH HHS/United States
- HD27917/HD/NICHD NIH HHS/United States
- U10 HD021410/HD/NICHD NIH HHS/United States
- U10 HD036801/HD/NICHD NIH HHS/United States
- U24 HD036801/HD/NICHD NIH HHS/United States
- U10 HD040545/HD/NICHD NIH HHS/United States
- HD40544/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
