

Value of Plasmodium falciparum histidine-rich protein 2 level and malaria retinopathy in distinguishing cerebral malaria from other acute encephalopathies in Kenyan children
- PMID: 24041795
- PMCID: PMC3903374
- DOI: 10.1093/infdis/jit500
Value of Plasmodium falciparum histidine-rich protein 2 level and malaria retinopathy in distinguishing cerebral malaria from other acute encephalopathies in Kenyan children
Abstract
Background: The diagnosis of cerebral malaria is problematic in malaria-endemic areas because encephalopathy in patients with parasitemia may have another cause. Abnormal retinal findings are thought to increase the specificity of the diagnosis, and the level of histidine-rich protein 2 (HRP2) may reflect the parasite biomass.
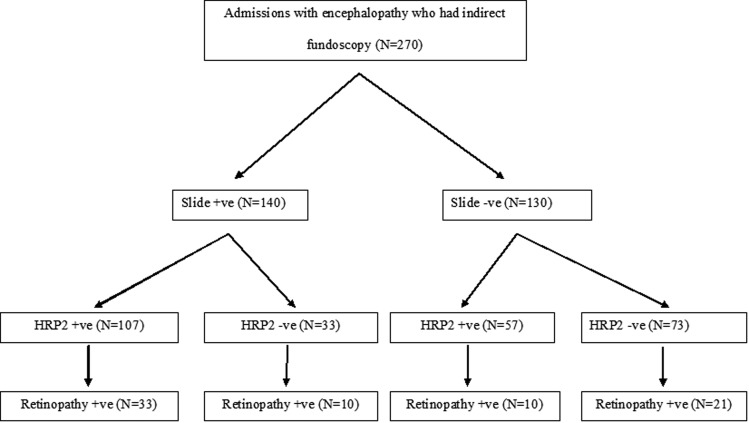
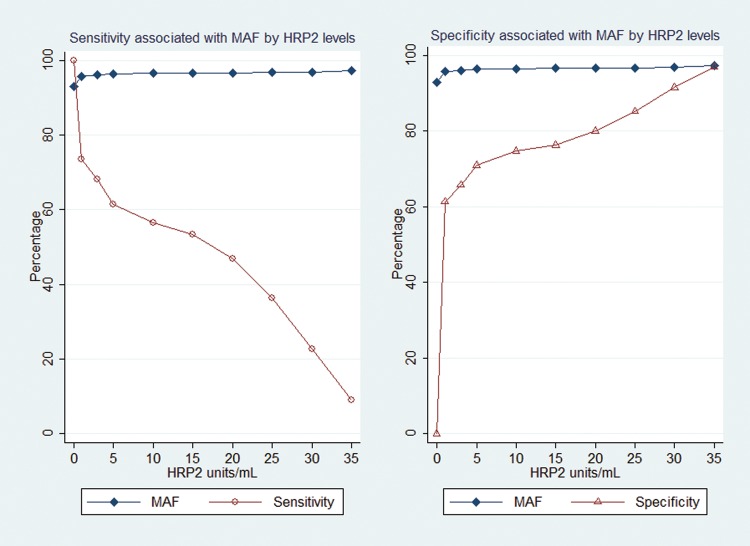
Methods: We examined the retina and measured plasma HRP2 levels in children with acute nontraumatic encephalopathy in Kenya. Logistic regression, with HRP2 level as an independent variable and World Health Organization-defined cerebral malaria and/or retinopathy as the outcome, was used to calculate malaria-attributable fractions (MAFs) and retinopathy-attributable fractions (RAFs).
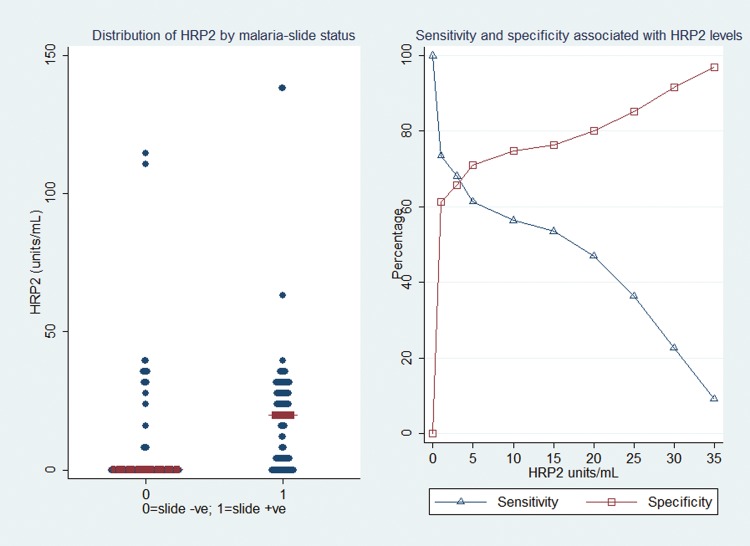
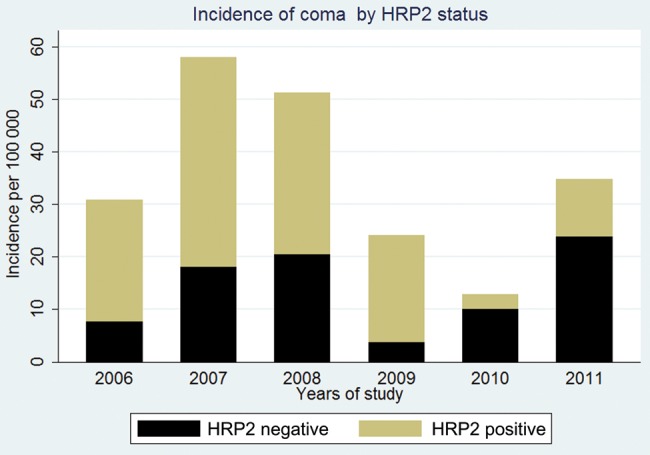
Results: Of 270 children, 140 (52%) had peripheral parasitemia, 80 (30%) had malaria retinopathy, and 164 (61%) had an HRP2 level of >0 U/mL. During 2006-2011, the incidence of HRP2 positivity among admitted children declined by 49 cases per 100 000 per year (a 78% reduction). An HRP2 level of >0 U/mL had a MAF of 93% for cerebral malaria, with a MAF of 97% observed for HRP2 levels of ≥ 10 U/mL (the level of the best combined sensitivity and specificity). HRP2 levels of >0 U/mL had a RAF of 77% for features of retinopathy combined, with the highest RAFs for macular whitening (99%), peripheral whitening (98%), and hemorrhages (90%).
Conclusion: HRP2 has a high attributable fraction for features of malarial retinopathy, supporting its use in the diagnosis of cerebral malaria. HRP2 thresholds improve the specificity of the definition.
Keywords: attributable fractions; cerebral malaria; children; histidine-rich protein-2; malaria retinopathy.
Figures
References
-
- Idro R, Jenkins NE, Newton CR. Pathogenesis, clinical features, and neurological outcome of cerebral malaria. Lancet Neurol. 2005;4:827–40. - PubMed
-
- World Health Organization. Severe falciparum malaria. Trans R Soc Trop Med Hyg. 2000;94:S1–90. - PubMed
-
- Snow RW, Omumbo JA, Lowe B, et al. Relation between severe malaria morbidity in children and level of Plasmodium falciparum transmission in Africa. Lancet. 1997;349:1650–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
