

Effects of four treatment strategies for temporomandibular joint closed lock
- PMID: 24042068
- PMCID: PMC3946573
- DOI: 10.1016/j.ijom.2013.07.744
Effects of four treatment strategies for temporomandibular joint closed lock
Abstract
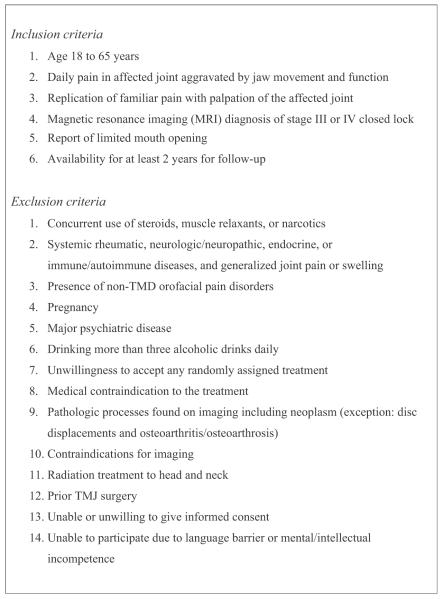
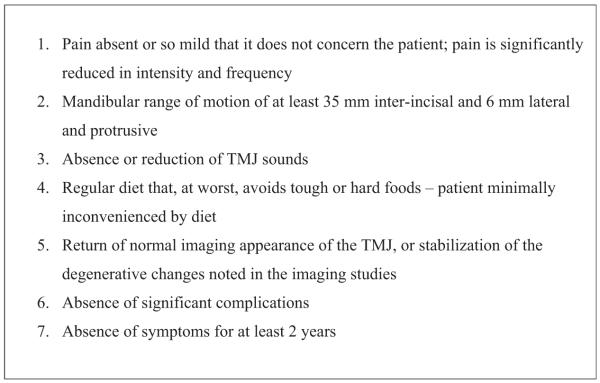
A previous randomized controlled trial (RCT) by Schiffman et al. (2007)(15) compared four treatments strategies for temporomandibular joint (TMJ) disc displacement without reduction with limited mouth opening (closed lock). In this parallel group RCT, 106 patients with magnetic resonance imaging (MRI)-confirmed TMJ closed lock were randomized between medical management, non-surgical rehabilitation, arthroscopic surgery, and arthroplasty. Surgical groups also received rehabilitation post-surgically. The current paper reassesses the effectiveness of these four treatment strategies using outcome measures recommended by the International Association of Oral and Maxillofacial Surgeons (IAOMS). Clinical assessments at baseline and at follow-up (3, 6, 12, 18, 24, and 60 months) included intensity and frequency of TMJ pain, mandibular range of motion, TMJ sounds, and impairment of chewing. TMJ MRIs were performed at baseline and 24 months, and TMJ tomograms at baseline, 24 and 60 months. Most IAOMS recommended outcome measures improved significantly over time (P≤0.0003). There was no difference between treatment strategies relative to any treatment outcome at any follow-up (P≥0.16). Patient self-assessment of treatment success correlated with their ability to eat, with pain-free opening ≥35mm, and with reduced pain intensity. Given no difference between treatment strategies, non-surgical treatment should be employed for TMJ closed lock before considering surgery.
Keywords: closed lock; randomized effectiveness study; surgery; temporomandibular joint; treatment success criteria.
Copyright © 2013 International Association of Oral and Maxillofacial Surgeons. All rights reserved.
Figures
Comment in
-
Importance of time as a factor in the management of temporomandibular joint closed lock.Int J Oral Maxillofac Surg. 2014 Oct;43(10):1302-3. doi: 10.1016/j.ijom.2014.07.003. Epub 2014 Jul 25. Int J Oral Maxillofac Surg. 2014. PMID: 25069852 No abstract available.
-
Response to letter to the editor--Temporomandibular joint closed lock.Int J Oral Maxillofac Surg. 2014 Oct;43(10):1303-4. doi: 10.1016/j.ijom.2014.07.002. Epub 2014 Jul 25. Int J Oral Maxillofac Surg. 2014. PMID: 25069853 No abstract available.
Similar articles
-
Discectomy without replacement for the treatment of painful reciprocal clicking or catching and chronic closed lock of the temporomandibular joint: a clinical follow-up audit.Br J Oral Maxillofac Surg. 2013 Dec;51(8):e211-4. doi: 10.1016/j.bjoms.2012.12.006. Epub 2013 Jan 29. Br J Oral Maxillofac Surg. 2013. PMID: 23369781
-
Randomized effectiveness study of four therapeutic strategies for TMJ closed lock.J Dent Res. 2007 Jan;86(1):58-63. doi: 10.1177/154405910708600109. J Dent Res. 2007. PMID: 17189464 Free PMC article. Clinical Trial.
-
Outcome of arthroscopic surgery for internal derangement of the temporomandibular joint: long-term results covering 10 years.J Craniomaxillofac Surg. 2000 Oct;28(5):264-71. doi: 10.1054/jcms.2000.0162. J Craniomaxillofac Surg. 2000. PMID: 11467389
-
Internal derangements of the temporomandibular joint: the role of arthroscopic surgery and arthrocentesis.J Can Dent Assoc. 2000 Apr;66(4):199-203. J Can Dent Assoc. 2000. PMID: 10789172 Review.
-
[Temporomandibular joint disc surgery].Rev Stomatol Chir Maxillofac Chir Orale. 2016 Sep;117(4):280-4. doi: 10.1016/j.revsto.2016.07.014. Epub 2016 Aug 17. Rev Stomatol Chir Maxillofac Chir Orale. 2016. PMID: 27544817 Review. French.
Cited by
-
Application of auriculotemporal nerve block and dextrose prolotherapy in exercise therapy of TMJ closed lock in adolescents and young adults.Head Face Med. 2021 Mar 27;17(1):11. doi: 10.1186/s13005-021-00261-7. Head Face Med. 2021. PMID: 33773589 Free PMC article.
-
Persistent Pain Following Proplast-Teflon Implants of the Temporomandibular Joint: A Case Report and 35-Year Management Perspective.J Pain Res. 2021 Sep 27;14:3033-3046. doi: 10.2147/JPR.S329123. eCollection 2021. J Pain Res. 2021. PMID: 34611434 Free PMC article.
-
A case of Melkersson-Rosenthal syndrome with temporomandibular joint osteoarthritis: multidisciplinary treatment and autoimmune etiological hypothesis.BMC Oral Health. 2024 Aug 13;24(1):935. doi: 10.1186/s12903-024-04723-7. BMC Oral Health. 2024. PMID: 39135018 Free PMC article.
-
Conservative versus Invasive Approaches in Temporomandibular Disc Displacement: A Systematic Review of Randomized Controlled Clinical Trials.Dent J (Basel). 2024 Jul 31;12(8):244. doi: 10.3390/dj12080244. Dent J (Basel). 2024. PMID: 39195088 Free PMC article. Review.
-
Impact of professional, recreational and nonsinging on temporomandibular disorders - a comparative study based on a self-assessment questionnaire.Head Face Med. 2024 Mar 21;20(1):19. doi: 10.1186/s13005-024-00419-z. Head Face Med. 2024. PMID: 38515168 Free PMC article.
References
-
- de Leeuw JR. Orofacial pain: guidelines for assessment, diagnosis, and management. Quintessence; Chicago, IL: 2008.
-
- Stegenga B, de Bont LG, Dijkstra PU, Boering G. Short-term outcome of arthroscopic surgery of temporomandibular joint osteoarthrosis and internal derangement: a randomized controlled clinical trial. Br J Oral Maxillofac Surg. 1993;31:3–14. - PubMed
-
- de Leeuw R, Boering G, Stegenga B, de Bont L. Temporomandibular joint osteoarthrosis: clinical and radiographic characteristics 30 years after nonsurgical treatment: a preliminary report. Cranio. 1993;11:15–24. - PubMed
-
- Rasmussen OC. Description of population and progress of symptoms in a longitudinal study of temporomandibular arthropathy. Scand J Dent Res. 1981;89:196–203. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
