

Comparative efficacy of in vitro and in vivo metabolized aspirin in the DeBakey ventricular assist device
- PMID: 24043375
- PMCID: PMC4160029
- DOI: 10.1007/s11239-013-0997-6
Comparative efficacy of in vitro and in vivo metabolized aspirin in the DeBakey ventricular assist device
Abstract
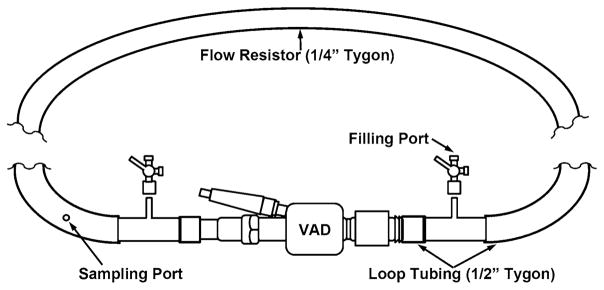
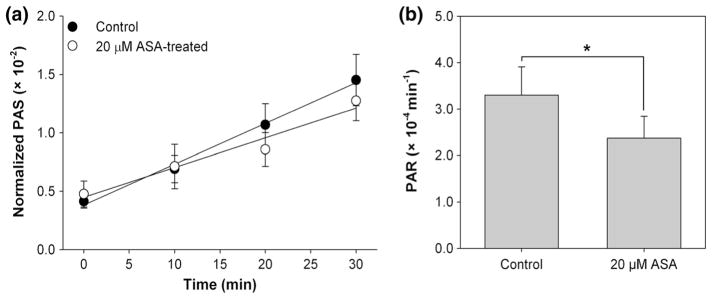
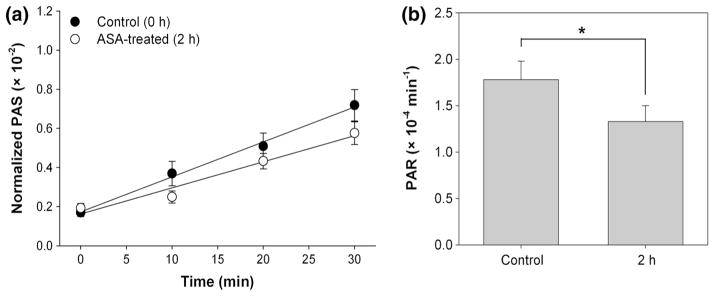
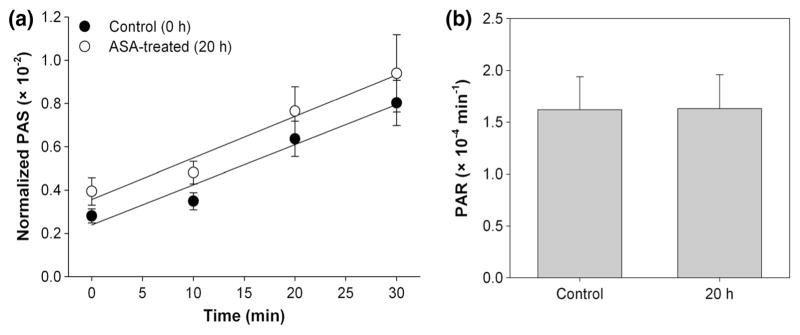
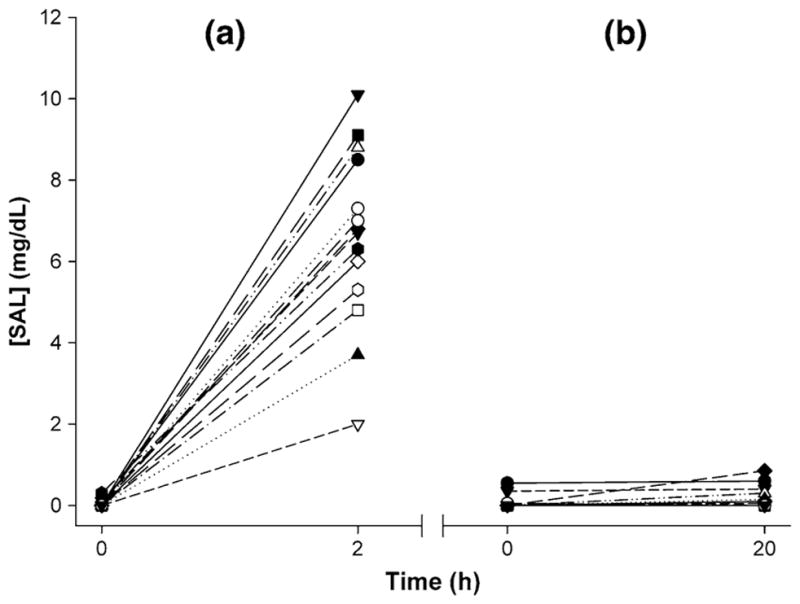
Ventricular assist devices (VADs) are implanted in patients with end-stage heart failure to provide both short- and long-term hemodynamic support. Unfortunately, bleeding and thromboembolic complications due to the severely disturbed, dynamic flow conditions generated within these devices require complex, long-term antiplatelet and anticoagulant therapy. While several studies have examined the effectiveness of one such agent, aspirin, under flow conditions, data comparing the efficacy of in vitro and in vivo metabolized aspirin is lacking. Two sets of studies were conducted in vitro with purified human platelets circulating for 30 min in a flow loop containing the DeBakey VAD (MicroMed Cardiovascular, Houston, TX, USA): (a) 20 μM aspirin was added exogenously in vitro to platelets isolated from aspirin-free subjects, and (b) platelets were obtained from donors 2 h (n = 14) and 20 h (n = 13) after ingestion of 1,000 mg aspirin. Near real-time platelet activation state (PAS) was measured with a modified prothrombinase-based assay. Platelets exposed to aspirin in vitro and in vivo (metabolized) showed 28.2 and 25.3 % reduction in platelet activation rate, respectively, compared to untreated controls. Our results demonstrate that in vitro treatment with antiplatelet drugs such as aspirin is as effective as in vivo metabolized aspirin in testing the effect of reducing shear-induced platelet activation in the VAD. Using the PAS assay provides a practical in vitro alternative to in vivo testing of antiplatelet efficacy, as well as for testing the thrombogenic performance of devices during their research and development.
Figures
Similar articles
-
Aspirin has limited ability to modulate shear-mediated platelet activation associated with elevated shear stress of ventricular assist devices.Thromb Res. 2016 Apr;140:110-117. doi: 10.1016/j.thromres.2016.01.026. Epub 2016 Feb 1. Thromb Res. 2016. PMID: 26938158 Free PMC article.
-
Routine clinical anti-platelet agents have limited efficacy in modulating hypershear-mediated platelet activation associated with mechanical circulatory support.Thromb Res. 2018 Mar;163:162-171. doi: 10.1016/j.thromres.2017.12.001. Epub 2017 Dec 5. Thromb Res. 2018. PMID: 29428715 Free PMC article.
-
Thromboresistance comparison of the HeartMate II ventricular assist device with the device thrombogenicity emulation- optimized HeartAssist 5 VAD.J Biomech Eng. 2014 Feb;136(2):021014. doi: 10.1115/1.4026254. J Biomech Eng. 2014. PMID: 24337144 Free PMC article.
-
A brief review on high on-aspirin residual platelet reactivity.Vascul Pharmacol. 2015 Apr-Jun;67-69:6-9. doi: 10.1016/j.vph.2015.03.018. Epub 2015 Apr 11. Vascul Pharmacol. 2015. PMID: 25869498 Review.
-
The genetics of antiplatelet drug resistance.Clin Genet. 2009 Jan;75(1):1-18. doi: 10.1111/j.1399-0004.2008.01105.x. Epub 2008 Nov 29. Clin Genet. 2009. PMID: 19067731 Review.
Cited by
-
Principles of TAVR valve design, modelling, and testing.Expert Rev Med Devices. 2018 Nov;15(11):771-791. doi: 10.1080/17434440.2018.1536427. Epub 2018 Oct 29. Expert Rev Med Devices. 2018. PMID: 30318937 Free PMC article. Review.
-
Physical Characterization and Platelet Interactions under Shear Flows of a Novel Thermoset Polyisobutylene-based Co-polymer.ACS Appl Mater Interfaces. 2015 Oct 7;7(39):22058-66. doi: 10.1021/acsami.5b07254. Epub 2015 Sep 23. ACS Appl Mater Interfaces. 2015. PMID: 26398588 Free PMC article.
-
Effects of Cone-Shaped Bend Inlet Cannulas of an Axial Blood Pump on Thrombus Formation: An Experiment and Simulation Study.Med Sci Monit. 2017 Apr 5;23:1655-1661. doi: 10.12659/msm.903421. Med Sci Monit. 2017. PMID: 28379938 Free PMC article.
-
Vibro-Acoustic Platelet Activation: An Additive Mechanism of Prothrombosis with Applicability to Snoring and Obstructive Sleep Apnea.Bioengineering (Basel). 2023 Dec 12;10(12):1414. doi: 10.3390/bioengineering10121414. Bioengineering (Basel). 2023. PMID: 38136005 Free PMC article.
-
Device Thrombogenicity Emulation: An In Silico Predictor of In Vitro and In Vivo Ventricular Assist Device Thrombogenicity.Sci Rep. 2019 Feb 27;9(1):2946. doi: 10.1038/s41598-019-39897-6. Sci Rep. 2019. PMID: 30814674 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
