

Adverse reactions to targeted and non-targeted chemotherapeutic drugs with emphasis on hypersensitivity responses and the invasive metastatic switch
- PMID: 24043487
- PMCID: PMC7102343
- DOI: 10.1007/s10555-013-9447-3
Adverse reactions to targeted and non-targeted chemotherapeutic drugs with emphasis on hypersensitivity responses and the invasive metastatic switch
Abstract
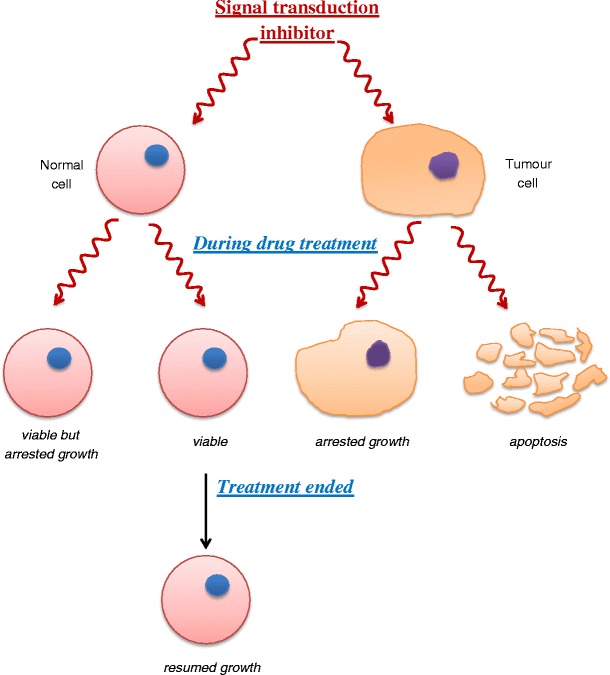
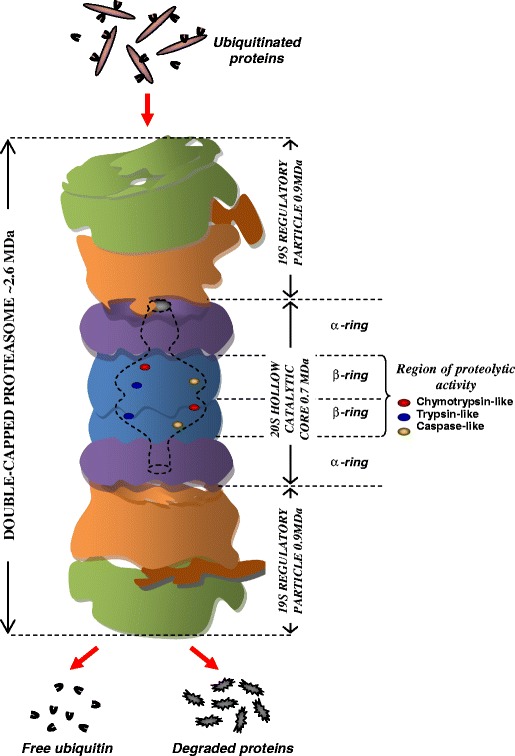
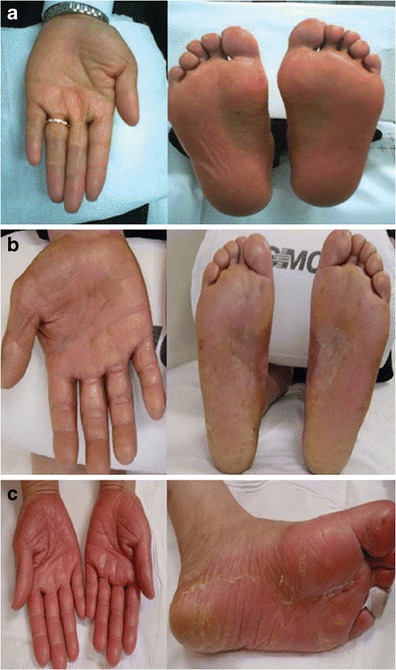
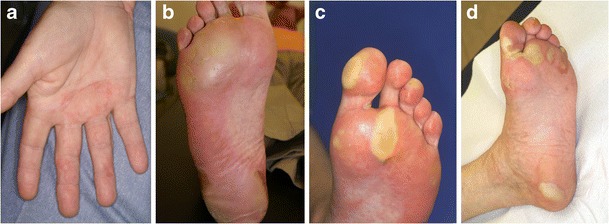
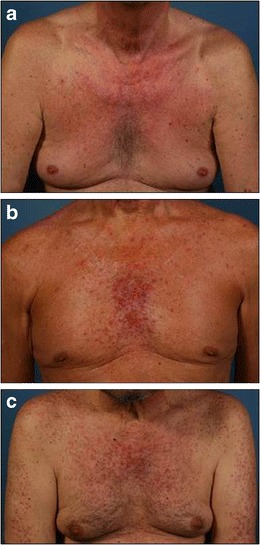
More than 100 drugs are used to treat the many different cancers. They can be divided into agents with relatively broad, non-targeted specificity and targeted drugs developed on the basis of a more refined understanding of individual cancers and directed at specific molecular targets on different cancer cells. Individual drugs in both groups have been classified on the basis of their mechanism of action in killing cancer cells. The targeted drugs include proteasome inhibitors, toxic chimeric proteins and signal transduction inhibitors such as tyrosine kinase (non-receptor and receptor), serine/threonine kinase, histone deacetylase and mammalian target of rapamycin inhibitors. Increasingly used targeted vascular (VEGF) and platelet-derived endothelial growth factor blockade can provoke a range of pathological consequences. Many of the non-targeted drugs are cytotoxic, suppressing haematopoiesis as well as provoking cutaneous eruptions and vascular, lung and liver injury. Cytotoxic side effects of the targeted drugs occur less often and usually with less severity, but they show their own unusual adverse effects including, for example, a lengthened QT interval, a characteristic papulopustular rash, nail disorders and a hand-foot skin reaction variant. The term hypersensitivity is widely used across a number of disciplines but not always with the same definition in mind, and the terminology needs to be standardised. This is particularly apparent in cancer chemotherapy where anti-neoplastic drug-induced thrombocytopenia, neutropenia, anaemia, vascular disorders, liver injury and lung disease as well as many dermatological manifestations sometimes have an immune basis. The most insidious of all adverse consequences of targeted therapies, however, are tumour adaptation, increased malignancy and the invasive metastatic switch seen with anti-angiogenic drugs that inhibit the VEGF-A pathway. Adverse reactions to 44 non-targeted and 33 targeted, frequently used, chemotherapeutic drugs are presented together with discussions of diagnosis, premedications, desensitizations and importance of understanding the mechanisms underlying the various drug-induced reactions. There is need for wide-ranging acceptance of what constitutes a hypersensitivity reaction and for allergists to be more involved in the diagnosis, treatment and prevention of chemotherapeutic drug-induced hypersensitivity reactions.
Figures
Similar articles
-
Adverse events to nontargeted and targeted chemotherapeutic agents: emphasis on hypersensitivity responses.Immunol Allergy Clin North Am. 2014 Aug;34(3):565-96, viii. doi: 10.1016/j.iac.2014.04.003. Immunol Allergy Clin North Am. 2014. PMID: 25017678 Review.
-
Rapid desensitization of hypersensitivity reactions to chemotherapy agents.Curr Drug Saf. 2006 Aug;1(3):243-51. doi: 10.2174/157488606777934413. Curr Drug Saf. 2006. PMID: 18690934 Review.
-
Desensitization for hypersensitivity reactions to medications.Chem Immunol Allergy. 2012;97:217-33. doi: 10.1159/000335637. Epub 2012 May 3. Chem Immunol Allergy. 2012. PMID: 22613865
-
Nonallergic drug hypersensitivity reactions.Int Arch Allergy Immunol. 2012;159(4):327-45. doi: 10.1159/000339690. Epub 2012 Jul 25. Int Arch Allergy Immunol. 2012. PMID: 22832422 Review.
-
Immediate Hypersensitivity Reaction to Chemotherapeutic Agents.J Allergy Clin Immunol Pract. 2017 May-Jun;5(3):593-599. doi: 10.1016/j.jaip.2017.03.015. J Allergy Clin Immunol Pract. 2017. PMID: 28483313 Review.
Cited by
-
Pharmaceutical and clinical studies of celecoxib topical hydrogel for management of chemotherapy-induced hand-foot syndrome.Naunyn Schmiedebergs Arch Pharmacol. 2023 Jul;396(7):1571-1581. doi: 10.1007/s00210-022-02339-8. Epub 2022 Nov 24. Naunyn Schmiedebergs Arch Pharmacol. 2023. PMID: 36418469 Clinical Trial.
-
Allergy in Cancer Care: Antineoplastic Therapy-Induced Hypersensitivity Reactions.Int J Mol Sci. 2023 Feb 15;24(4):3886. doi: 10.3390/ijms24043886. Int J Mol Sci. 2023. PMID: 36835299 Free PMC article. Review.
-
2-Arachidonoylglycerol enhances platelet formation from human megakaryoblasts.Cell Cycle. 2014;13(24):3938-47. doi: 10.4161/15384101.2014.982941. Cell Cycle. 2014. PMID: 25427281 Free PMC article.
-
Cisplatin-induced sudden cardiac death with hemodynamic collapse: a severe adverse drug reaction: Case report.Medicine (Baltimore). 2017 Dec;96(48):e8995. doi: 10.1097/MD.0000000000008995. Medicine (Baltimore). 2017. PMID: 29310415 Free PMC article.
-
Incidence of infusion reactions to anti-neoplastic agents in early phase clinical trials: The MD Anderson Cancer Center experience.Invest New Drugs. 2017 Feb;35(1):59-67. doi: 10.1007/s10637-016-0395-y. Epub 2016 Sep 29. Invest New Drugs. 2017. PMID: 27687047 Free PMC article.
References
-
- World Health Organization. (1972). International drug monitoring: the role of national centres. WHO Technical Report Series, no. 498, pp. 1–25. - PubMed
-
- Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet. 2000;356(9237):1255–1259. - PubMed
-
- What is a serious event? http:/www.fda.gov/safety/medwatch/howtoreport/ucm053087.htm. Accessed 18 February 2013.
-
- Meyer UA. Pharmacogenetics and adverse drug reactions. Lancet. 2000;356(9237):1667–1671. - PubMed
-
- Coombs RRA, Gell PGH. Classification of allergic reactions responsible for clinical hypersensitivity and disease. In: Gell PGH, Coombs RRA, Lachmann PJ, editors. Clinical aspects of immunology. Oxford: Blackwell; 1975. pp. 761–781.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
