

Is mTOR inhibition a systemic treatment for tuberous sclerosis?
- PMID: 24044547
- PMCID: PMC3848592
- DOI: 10.1186/1824-7288-39-57
Is mTOR inhibition a systemic treatment for tuberous sclerosis?
Abstract
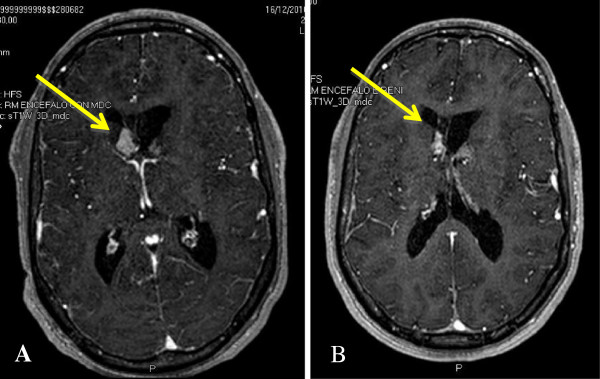
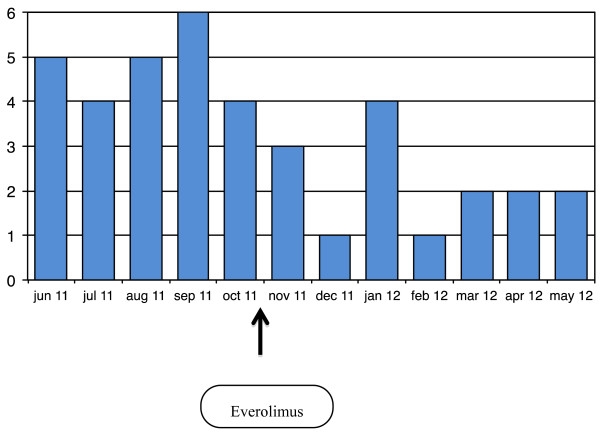
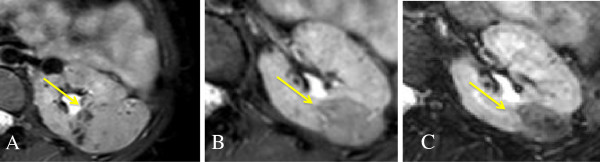
Tuberous sclerosis complex (TSC) is a genetic multisystem disorder characterized by the development of hamartomas in several organs. Mutations in the TSC1 and TSC2 tumor suppressor genes determin overactivation of the mammalian target of rapamycin (mTOR) signaling pathway and subsequent abnormalities in numerous cell processes. As a result, mTOR inhibitors such as sirolimus and everolimus have the potential to provide targeted therapy for TSC patients. Everolimus has been recently approved as a pharmacotherapy option for TSC patients with subependymal giant-cell astrocytomas (SEGAs) or renal angiomyolipomas (AMLs). However, clinical evidence suggests that this treatment can benefit other TSC-associated disease manifestations, such as skin manifestations, pulmonary lymphangioleiomyomatosis, cardiac rhabdomyomas, and epilepsy. Therefore, the positive effects that mTOR inhibition have on a wide variety of TSC disease manifestations make this a potential systemic treatment option for this genetic multifaceted disorder.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
