

Allopregnanolone as regenerative therapeutic for Alzheimer's disease: translational development and clinical promise
- PMID: 24044981
- PMCID: PMC10124616
- DOI: 10.1016/j.pneurobio.2013.08.004
Allopregnanolone as regenerative therapeutic for Alzheimer's disease: translational development and clinical promise
Abstract
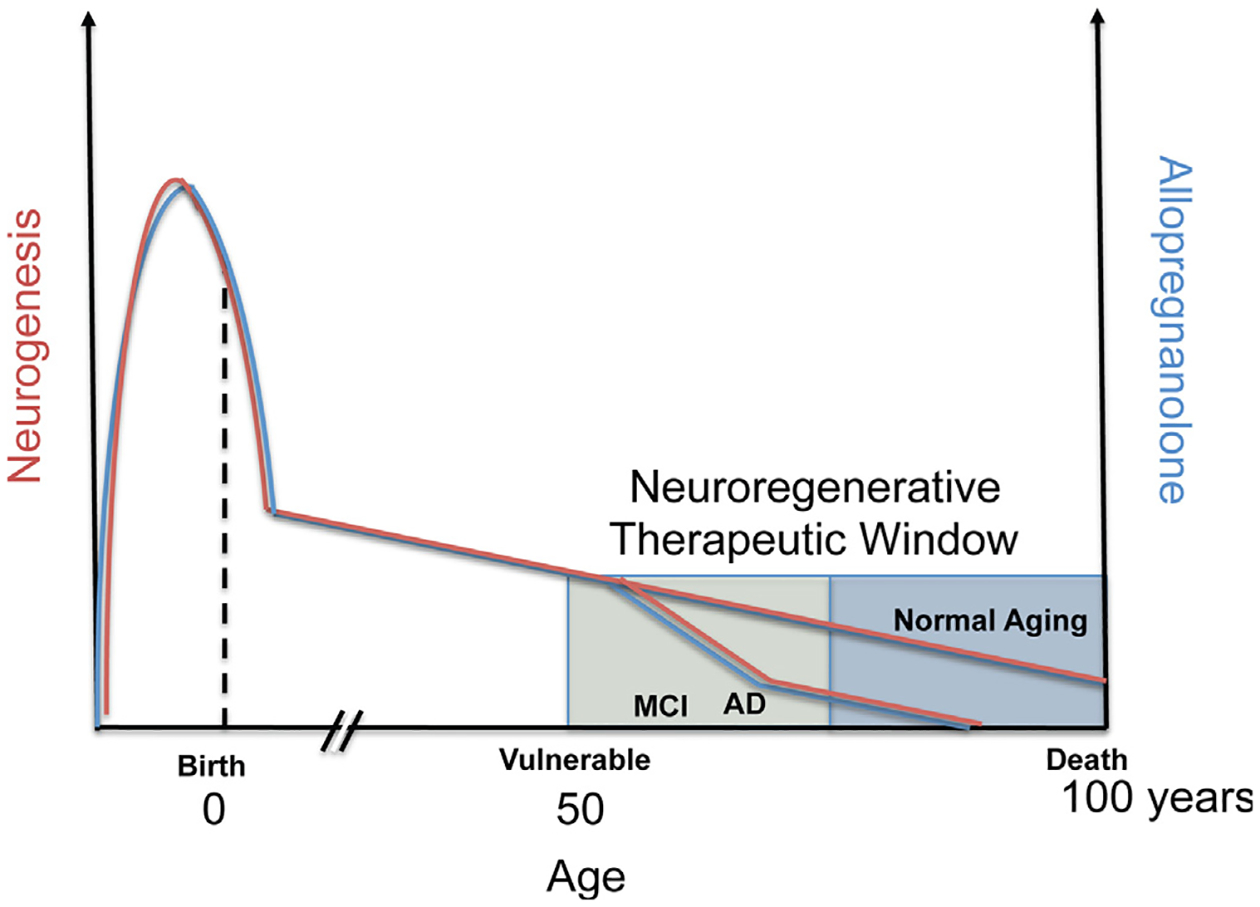
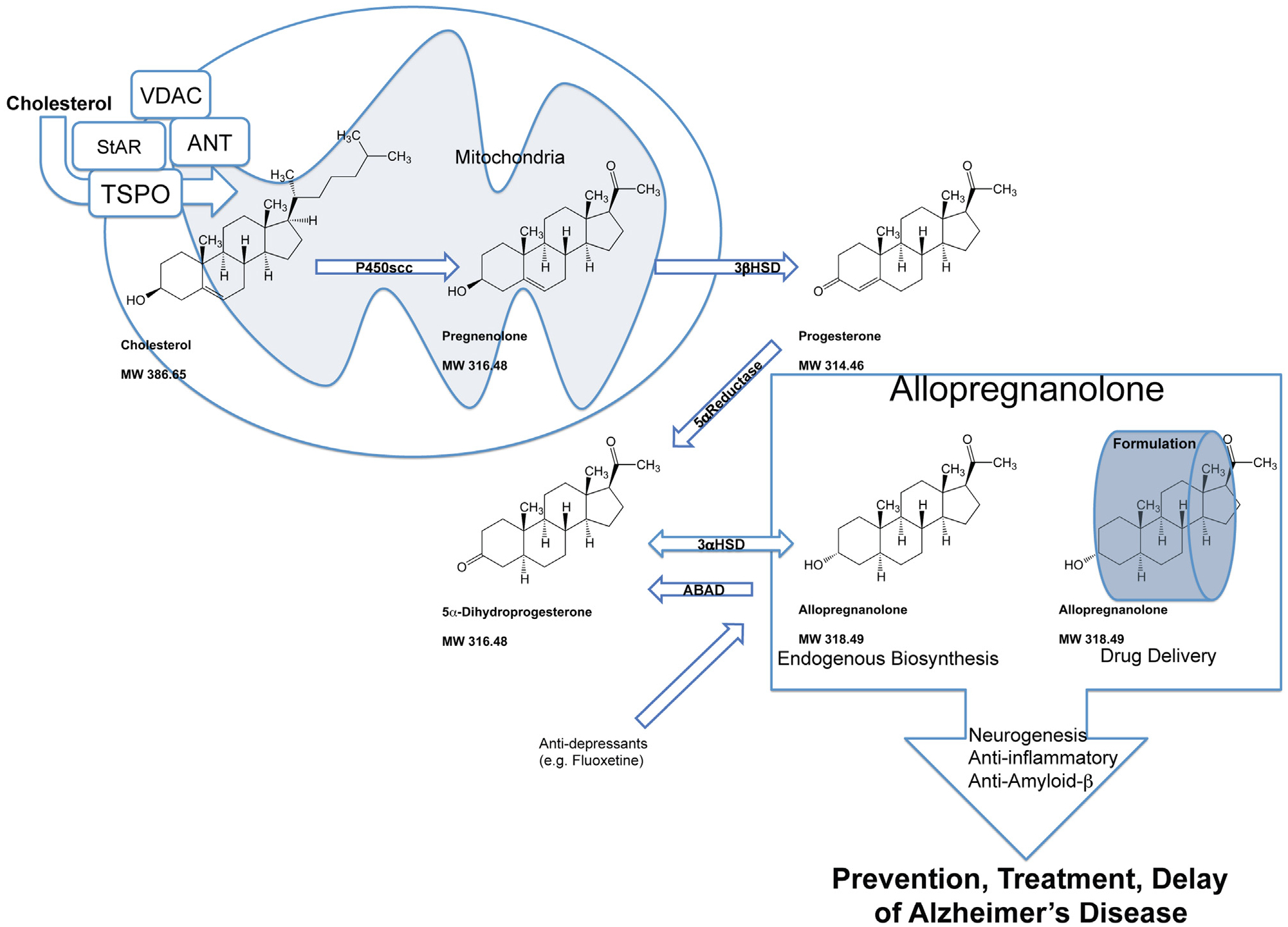
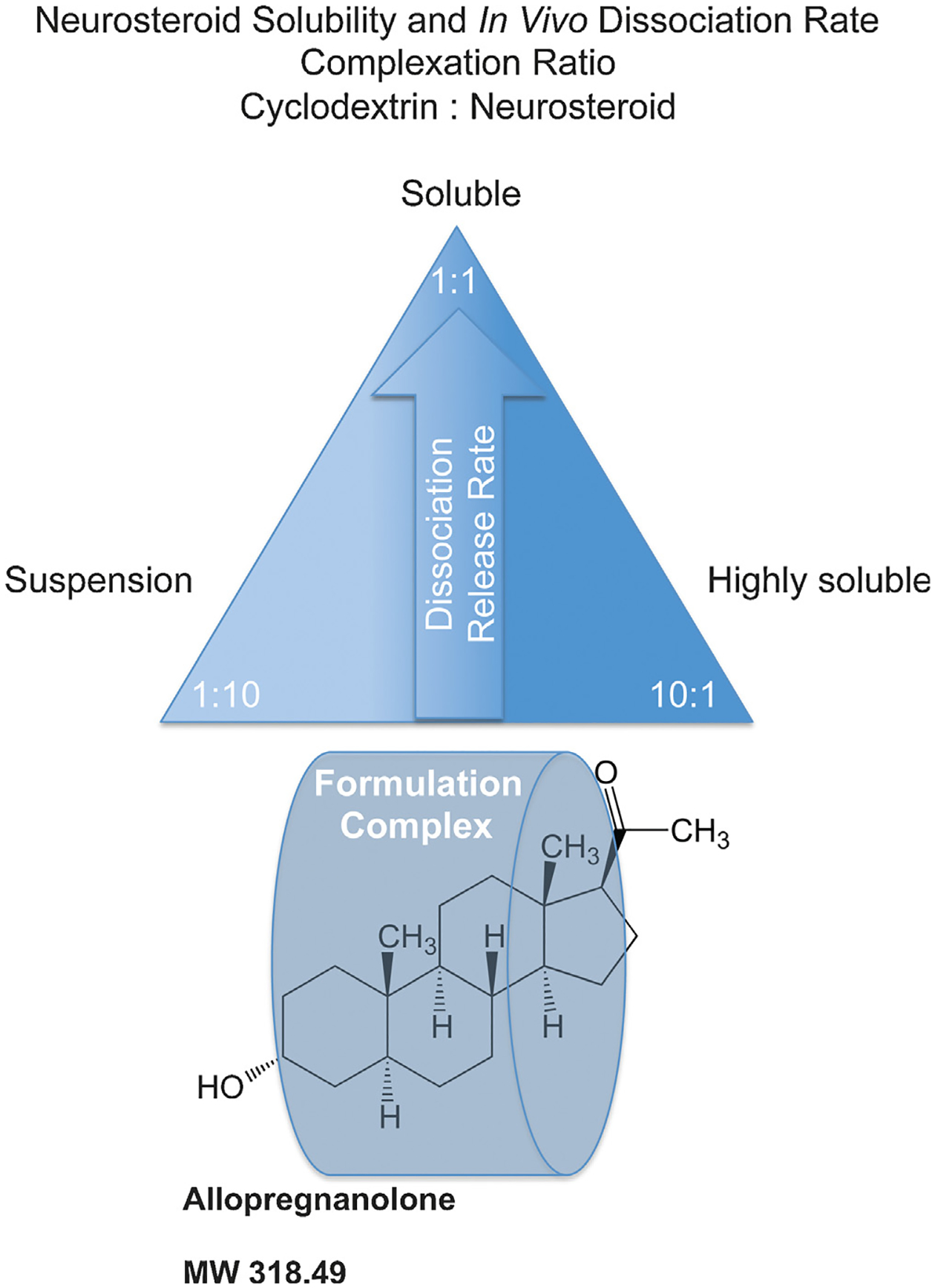
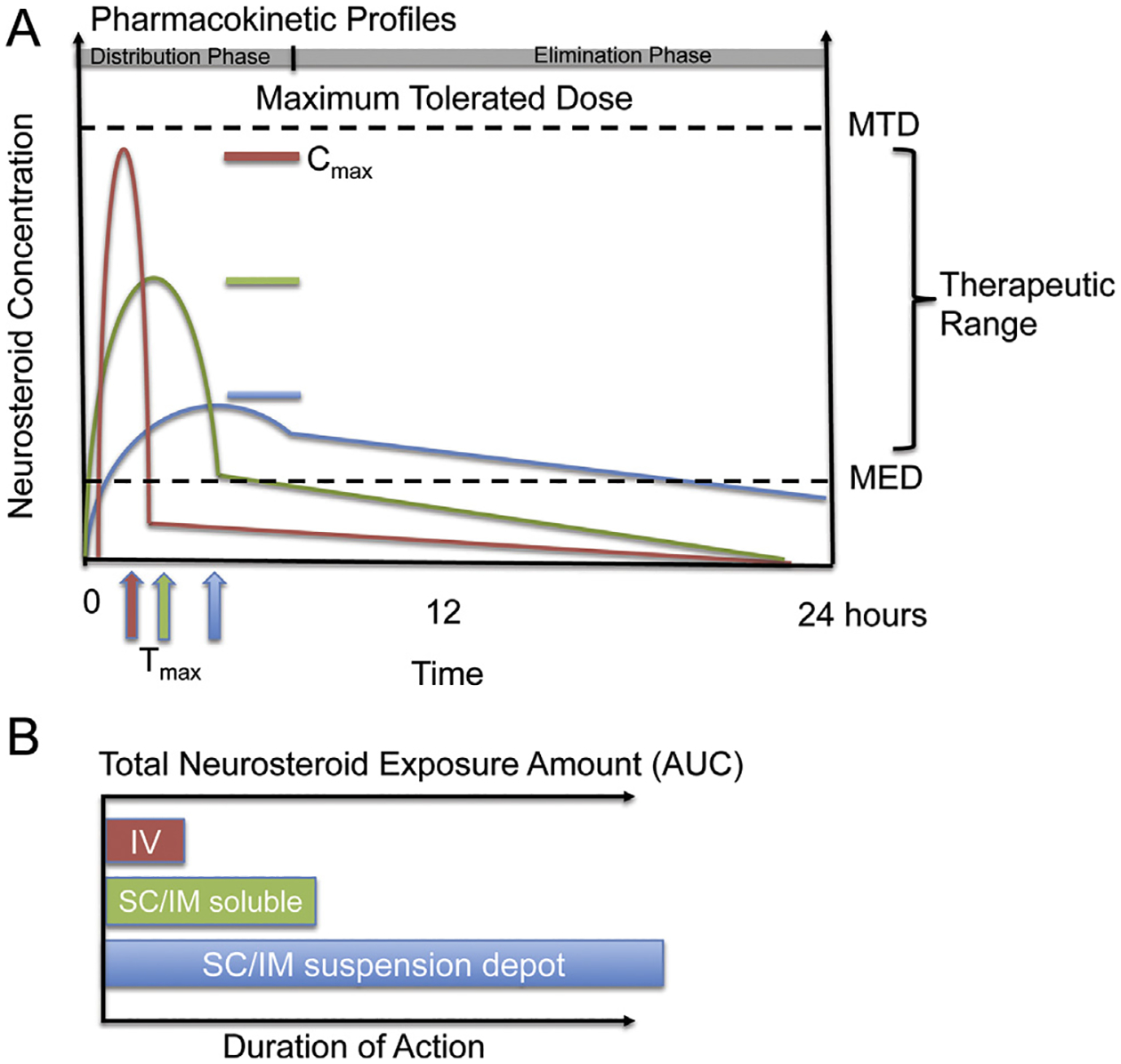
Herein, we review a translational development plan to advance allopregnanolone to the clinic as a regenerative therapeutic for neurodegenerative diseases, in particular Alzheimer's. Allopregnanolone, an endogenous neurosteroid that declines with age and neurodegenerative disease, was exogenously administered and assessed for safety and efficacy to promote neuro-regeneration, cognitive function and reduction of Alzheimer's pathology. Allopregnanolone-induced neurogenesis correlated with restoration of learning and memory function in a mouse model of Alzheimer's disease and was comparably efficacious in aged normal mice. Critical to success was a dosing and treatment regimen that was consistent with the temporal requirements of systems biology of regeneration in brain. A treatment regimen that adhered to regenerative requirements of brain was also efficacious in reducing Alzheimer's pathology. With an optimized dosing and treatment regimen, chronic allopregnanolone administration promoted neurogenesis, oligodendrogenesis, reduced neuroinflammation and beta-amyloid burden while increasing markers of white matter generation and cholesterol homeostasis. Allopregnanolone meets three of the four drug-like physicochemical properties described by Lipinski's rule that predict the success rate of drugs in development for clinical trials. Pharmacokinetic and pharmacodynamic outcomes, securing GMP material, development of clinically translatable formulations and acquiring regulatory approval are discussed. Investigation of allopregnanolone as a regenerative therapeutic has provided key insights into mechanistic targets for neurogenesis and disease modification, dosing requirements, optimal treatment regimen, route of administration and the appropriate formulation necessary to advance to proof of concept clinical studies to determine efficacy of allopregnanolone as a regenerative and disease modifying therapeutic for Alzheimer's disease.
Keywords: 2-hydroxypropyl β-cyclodextrin; 3-hydroxy-3-methyl-glutaryl-CoA-reductase; 3xTgAD; 3α-HSD; 3α-hydroxysteroid dehydrogenase; 3β-HSD; 3β-hydroxysteroid dehydrogenase; 5α-DHP; 5α-R; 5α-dihydroprogesterone; 5α-reductase; ABAD; AD; ANT; AUC; Allo; Alzheimer's disease; Aβ; CMC; CYP3A; CYP450scc; EMA; European Medicines Agency; FDA; GLP; Good Laboratory Practices; Good Manufacturing Practices; HMG-CoA-R; HβCD; IM; IN; IND; IV; LXR; MED; MTD; Neurogenesis; Neurosteroid; PKA; PKCɛ; PXR; Pharmacodynamics; Pharmacokinetics; Regenerative medicine; SBEβCD; SC; SGZ; SVZ; StAR; TD; TSPO; Treatment regimen; United States Food and Drug Administration; VDAC; adenine nucleotide transporter protein; allopregnanolone; amyloid-beta binding alcohol dehydrogenase; area under the curve; cGMP; chemistry, manufacturing, and controls; cytochrome P450 3A; cytochrome P450 side-chain cleavage; intramuscular; intranasal; intravenous; investigational new drug; liver-X-receptor; maximum tolerated dose; minimal effective dose; non-transgenic; nonTg; pregnane-X-receptor; protein kinase A; protein kinase C epsilon; steroidogenic acute regulatory protein; subcutaneous; subgranular zone; subventricular zone; sulfobutyl ether β-cyclodextrin; transdermal; translocator protein; triple transgenic mouse model of AD; voltage-dependent anion channel protein; β-amyloid.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Allopregnanolone preclinical acute pharmacokinetic and pharmacodynamic studies to predict tolerability and efficacy for Alzheimer's disease.PLoS One. 2015 Jun 3;10(6):e0128313. doi: 10.1371/journal.pone.0128313. eCollection 2015. PLoS One. 2015. PMID: 26039057 Free PMC article.
-
Allopregnanolone promotes regeneration and reduces β-amyloid burden in a preclinical model of Alzheimer's disease.PLoS One. 2011;6(8):e24293. doi: 10.1371/journal.pone.0024293. Epub 2011 Aug 30. PLoS One. 2011. PMID: 21918687 Free PMC article.
-
Neuroregenerative mechanisms of allopregnanolone in Alzheimer's disease.Front Endocrinol (Lausanne). 2012 Jan 12;2:117. doi: 10.3389/fendo.2011.00117. eCollection 2011. Front Endocrinol (Lausanne). 2012. PMID: 22654847 Free PMC article.
-
Preclinical analyses of the therapeutic potential of allopregnanolone to promote neurogenesis in vitro and in vivo in transgenic mouse model of Alzheimer's disease.Curr Alzheimer Res. 2006 Feb;3(1):11-7. doi: 10.2174/156720506775697160. Curr Alzheimer Res. 2006. PMID: 16472197 Review.
-
Neurosteroids as regenerative agents in the brain: therapeutic implications.Nat Rev Endocrinol. 2013 Apr;9(4):241-50. doi: 10.1038/nrendo.2013.31. Epub 2013 Feb 26. Nat Rev Endocrinol. 2013. PMID: 23438839 Free PMC article. Review.
Cited by
-
Progesterone in the Brain: Hormone, Neurosteroid and Neuroprotectant.Int J Mol Sci. 2020 Jul 24;21(15):5271. doi: 10.3390/ijms21155271. Int J Mol Sci. 2020. PMID: 32722286 Free PMC article. Review.
-
Homocysteine, Cognitive Functions, and Degenerative Dementias: State of the Art.Biomedicines. 2022 Oct 28;10(11):2741. doi: 10.3390/biomedicines10112741. Biomedicines. 2022. PMID: 36359260 Free PMC article. Review.
-
Light-at-night exposure affects brain development through pineal allopregnanolone-dependent mechanisms.Elife. 2019 Sep 30;8:e45306. doi: 10.7554/eLife.45306. Elife. 2019. PMID: 31566568 Free PMC article.
-
Golexanolone, a GABAA receptor modulating steroid antagonist, restores motor coordination and cognitive function in hyperammonemic rats by dual effects on peripheral inflammation and neuroinflammation.CNS Neurosci Ther. 2022 Nov;28(11):1861-1874. doi: 10.1111/cns.13926. Epub 2022 Jul 26. CNS Neurosci Ther. 2022. PMID: 35880480 Free PMC article.
-
Cellular cholesterol homeostasis and Alzheimer's disease.J Lipid Res. 2017 Dec;58(12):2239-2254. doi: 10.1194/jlr.R075630. Epub 2017 Mar 15. J Lipid Res. 2017. PMID: 28298292 Free PMC article. Review.
References
-
- Altman J, 1969. Autoradiographic and histological studies of postnatal neurogenesis. IV. Cell proliferation and migration in the anterior forebrain, with special reference to persisting neurogenesis in the olfactory bulb. J. Comp. Neurol 137, 433–457. - PubMed
-
- Altman J, Das GD, 1965. Autoradiographic and histological evidence of postnatal hippocampal neurogenesis in rats. J. Comp. Neurol 124, 319–335. - PubMed
-
- Alzheimer’s Association, 2013. Alzheimer’s Disease Facts and Figures. - PubMed
-
- Alzheimer’s Disease International, 2012. World Alzheimer Report 2012: Overcoming the Stigma of Dementia
-
- Barbaccia ML, Roscetti G, Trabucchi M, Cuccheddu T, Concas A, Biggio G, 1994. Neurosteroids in the brain of handling-habituated and naive rats: effect of CO2 inhalation. Eur. J. Pharmacol 261, 317–320. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
