

Randomized trial of conventional transseptal needle versus radiofrequency energy needle puncture for left atrial access (the TRAVERSE-LA study)
- PMID: 24045120
- PMCID: PMC3835257
- DOI: 10.1161/JAHA.113.000428
Randomized trial of conventional transseptal needle versus radiofrequency energy needle puncture for left atrial access (the TRAVERSE-LA study)
Abstract
Background: Transseptal puncture is a critical step in achieving left atrial (LA) access for a variety of cardiac procedures. Although the mechanical Brockenbrough needle has historically been used for this procedure, a needle employing radiofrequency (RF) energy has more recently been approved for clinical use. We sought to investigate the comparative effectiveness of an RF versus conventional needle for transseptal LA access.
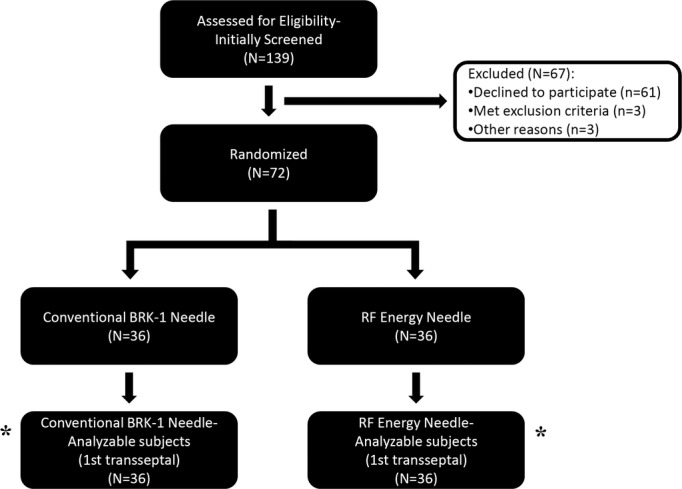
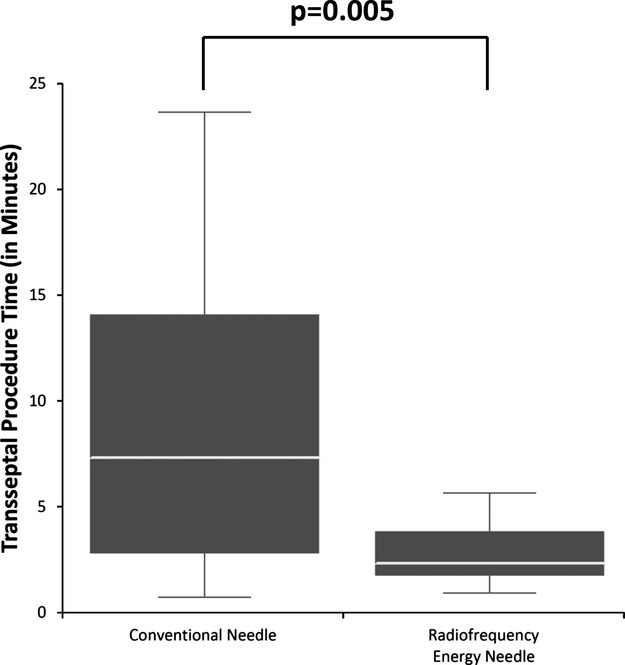
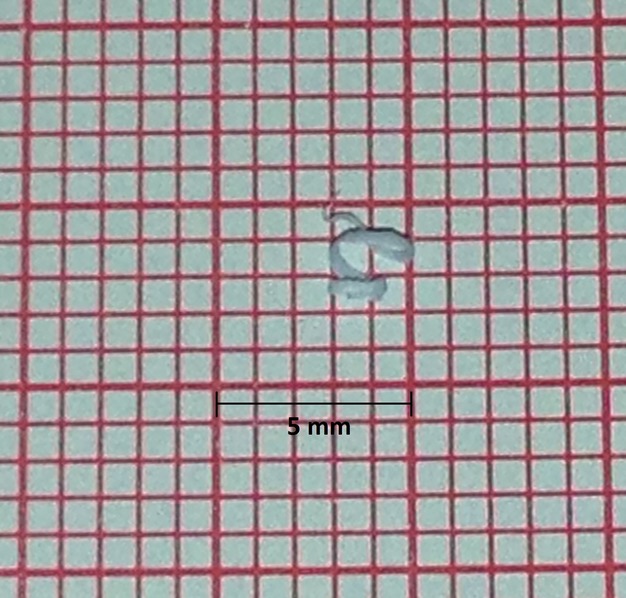
Methods and results: In this prospective, single-blinded, controlled trial, 72 patients were randomized in a 1:1 fashion to an RF versus conventional (BRK-1) transseptal needle. In an intention-to-treat analysis, the primary outcome was time required for transseptal LA access. Secondary outcomes included failure of the assigned needle, visible plastic dilator shavings from needle introduction, and any procedural complication. The median transseptal puncture time was 68% shorter using the RF needle compared with the conventional needle (2.3 minutes [interquartile range {IQR}, 1.7 to 3.8 minutes] versus 7.3 minutes [IQR, 2.7 to 14.1 minutes], P = 0.005). Failure to achieve transseptal LA access with the assigned needle was less common using the RF versus conventional needle (0/36 [0%] versus 10/36 [27.8%], P < 0.001). Plastic shavings were grossly visible after needle advancement through the dilator and sheath in 0 (0%) RF needle cases and 12 (33.3%) conventional needle cases (P < 0.001). There were no differences in procedural complications (1/36 [2.8%] versus 1/36 [2.8%]).
Conclusions: Use of an RF needle resulted in shorter time to transseptal LA access, less failure in achieving transseptal LA access, and fewer visible plastic shavings.
Trial registration: ClinicalTrials.gov NCT01209260.
Keywords: Brockenbrough needle; comparative effectiveness; left atrial access; radiofrequency energy needle; randomized controlled trial; transseptal puncture.
Figures
References
-
- Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, Crijns HJ, Damiano RJ, Jr, Davies DW, DiMarco J, Edgerton J, Ellenbogen K, Ezekowitz MD, Haines DE, Haissaguerre M, Hindricks G, Iesaka Y, Jackman W, Jalife J, Jais P, Kalman J, Keane D, Kim YH, Kirchhof P, Klein G, Kottkamp H, Kumagai K, Lindsay BD, Mansour M, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Nakagawa H, Natale A, Nattel S, Packer DL, Pappone C, Prystowsky E, Raviele A, Reddy V, Ruskin JN, Shemin RJ, Tsao HM, Wilber D. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow‐up, definitions, endpoints, and research trial design. J Interv Card Electrophysiol. 2012; 33:171-257 - PubMed
-
- Lesh MD, Van Hare GF, Scheinman MM, Ports TA, Epstein LA. Comparison of the retrograde and transseptal methods for ablation of left free wall accessory pathways. J Am Coll Cardiol. 1993; 22:542-549 - PubMed
-
- Pluta S, Lenarczyk R, Pruszkowska‐Skrzep P, Kowalski O, Sokal A, Sredniawa B, Mazurek M, Kalarus Z. Transseptal versus transaortic approach for radiofrequency ablation in patients with cardioverter‐defibrillator and electrical storm. J Interv Card Electrophysiol. 2010; 28:45-50 - PubMed
-
- Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, Mullin CM, Sick P. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non‐inferiority trial. Lancet. 2009; 374:534-542 - PubMed
-
- Bartus K, Han FT, Bednarek J, Myc J, Kapelak B, Sadowski J, Lelakowski J, Bartus S, Yakubov SJ, Lee RJ. Percutaneous left atrial appendage suture ligation using the lariat device in patients with atrial fibrillation: initial clinical experience. J Am Coll Cardiol. 2013; 62:108-118 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
