

Emergency presentation of cancer and short-term mortality
- PMID: 24045658
- PMCID: PMC3798965
- DOI: 10.1038/bjc.2013.569
Emergency presentation of cancer and short-term mortality
Abstract
Background: The short-term survival following a cancer diagnosis in England is lower than that in comparable countries, with the difference in excess mortality primarily occurring in the months immediately after diagnosis. We assess the impact of emergency presentation (EP) on the excess mortality in England over the course of the year following diagnosis.
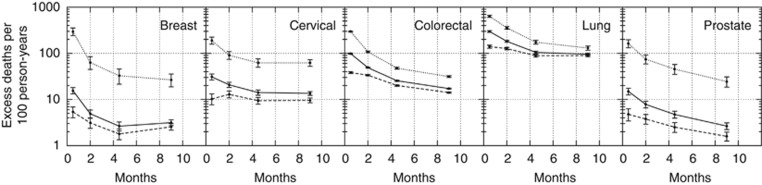
Methods: All colorectal and cervical cancers presenting in England and all breast, lung, and prostate cancers in the East of England in 2006-2008 are included. The variation in the likelihood of EP with age, stage, sex, co-morbidity, and income deprivation is modelled. The excess mortality over 0-1, 1-3, 3-6, and 6-12 months after diagnosis and its dependence on these case-mix factors and presentation route is then examined.
Results: More advanced stage and older age are predictive of EP, as to a lesser extent are co-morbidity, higher income deprivation, and female sex. In the first month after diagnosis, we observe case-mix-adjusted excess mortality rate ratios of 7.5 (cervical), 5.9 (colorectal), 11.7 (breast ), 4.0 (lung), and 20.8 (prostate) for EP compared with non-EP.
Conclusion: Individuals who present as an emergency experience high short-term mortality in all cancer types examined compared with non-EPs. This is partly a case-mix effect but EP remains predictive of short-term mortality even when age, stage, and co-morbidity are accounted for.
Figures
References
-
- Berrino F, De Angelis R, Sant M, Rosso S, Lasota MB, Coebergh JWW, Santaquilani M, EUROCARE Working Group Survival for eight major cancers and all cancers combined for European adults diagnosed in 1995 –1999: results of the EUROCARE-4 study. Lancet Oncol. 2007;8:773–783. - PubMed
-
- Blaney J, Gavin A. Why cancer patients die in acute hospitals: a retrospective study by note review. N Ireland Cancer Registry. 2011.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
