

Fibula head is a useful landmark to predict the location of posterior cruciate ligament footprint prior to total knee arthroplasty
- PMID: 24045910
- PMCID: PMC3923929
- DOI: 10.1007/s00264-013-2100-5
Fibula head is a useful landmark to predict the location of posterior cruciate ligament footprint prior to total knee arthroplasty
Abstract
Purpose: The hypothesis of our study is that a routine tibial cut during cruciate retaining TKA may result in a partial or a total removal of the PCL footprint. Therefore providing a reliable landmark is essential to estimate the probability of PCL damage with a tibial cut and to enable the surgeon to decide pre-operatively whether a cruciate retaining implant design is suitable.
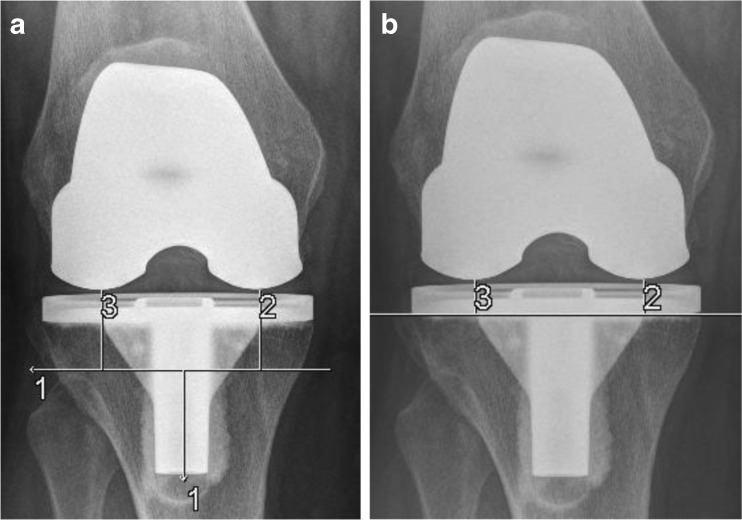
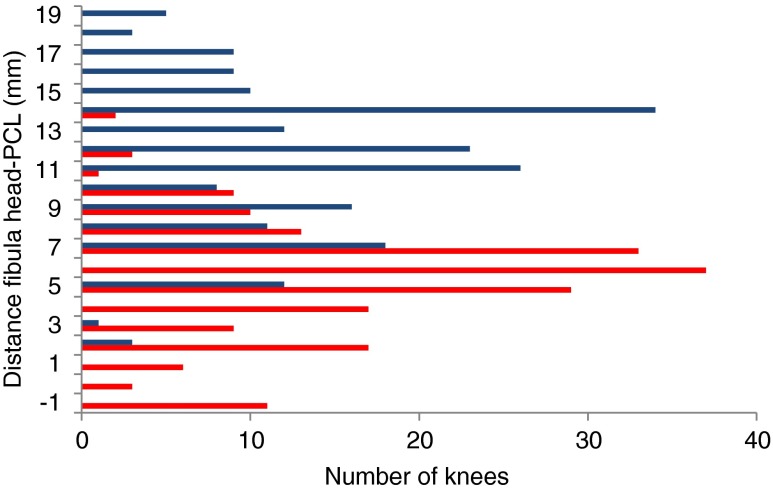
Methods: In a case series of 175 cruciate retaining TKA, the routinely made standing postoperative AP-view radiographs were evaluated to determine the distance between fibula head and tibial cutting plane. In a second case series knee MRI of 223 subjects were consecutively used to measure the vertical distance between tibial attachment of PCL and fibula head. The probability of partial or total PCL damage was calculated for different vertical distances between tibial cut and fibula head.
Results: The vertical distance between the tibial cut and the most proximal point of the fibula head averaged 6.1 mm ±4.8 mm. The mean vertical distance from fibula head to proximal and to distal PCL footprint revealed to be 11.4 mm ±3.7 mm and 5.4 mm ±2.9 mm, respectively. The location of the insertion was not significantly different between subgroups such as age (<50 or >50 years), gender and side. Based on our results 11 (7%) knees were considered at high risk of an entire PCL removal after implantation of a cruciate retaining TKA design.
Conclusions: Currently available routine tibial preparation techniques result in partial or total posterior cruciate ligament detachment. Fibula head as a landmark aids to predict the PCL location and to estimate its disruption pre- and postoperatively on AP-view radiographs.
Figures



Similar articles
-
Preservation of the PCL when performing cruciate-retaining TKA: Is the tibial tuberosity a reliable predictor of the PCL footprint location?Knee Surg Sports Traumatol Arthrosc. 2016 Jan;24(1):58-63. doi: 10.1007/s00167-014-3309-6. Epub 2014 Sep 14. Knee Surg Sports Traumatol Arthrosc. 2016. PMID: 25218577
-
Cruciate-retaining total knee arthroplasty: How much of the PCL is really retained?Knee Surg Sports Traumatol Arthrosc. 2017 Nov;25(11):3556-3560. doi: 10.1007/s00167-016-4144-8. Epub 2016 May 3. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 27141866
-
The posterior cruciate ligament-preserving total knee replacement: do we 'preserve' it? A radiological study.J Bone Joint Surg Br. 2007 Jun;89(6):766-71. doi: 10.1302/0301-620X.89B6.18782. J Bone Joint Surg Br. 2007. PMID: 17613501
-
Current evidence advocates use of a new pathologic tibial tubercle-posterior cruciate ligament distance threshold in patients with patellar instability.Knee Surg Sports Traumatol Arthrosc. 2018 Sep;26(9):2733-2742. doi: 10.1007/s00167-017-4716-2. Epub 2017 Sep 16. Knee Surg Sports Traumatol Arthrosc. 2018. PMID: 28918500
-
Rupture of the Posterior Cruciate Ligament: Preoperative and Postoperative Assessment.Semin Musculoskelet Radiol. 2016 Feb;20(1):43-51. doi: 10.1055/s-0036-1579711. Epub 2016 Apr 14. Semin Musculoskelet Radiol. 2016. PMID: 27077586 Review.
Cited by
-
Knee joint line related to bony landmarks of the knee: a radiologic study in a Thai population.Knee Surg Relat Res. 2022 Feb 15;34(1):5. doi: 10.1186/s43019-022-00135-5. Knee Surg Relat Res. 2022. PMID: 35168654 Free PMC article.
-
Knee arthroplasty today.Int Orthop. 2014 Feb;38(2):221-5. doi: 10.1007/s00264-013-2274-x. Int Orthop. 2014. PMID: 24420157 Free PMC article. No abstract available.
-
The predictive effect of anatomic femoral and tibial graft tunnel placement in posterior cruciate ligament reconstruction on functional and radiological outcome.Int Orthop. 2015 Jun;39(6):1181-6. doi: 10.1007/s00264-014-2565-x. Epub 2014 Oct 18. Int Orthop. 2015. PMID: 25324225
-
Correlation between varus-type knee osteoarthritis severity and hindfoot alignment: Analysis of radiographs in the long-leg weight-bearing anteroposterior view.PLoS One. 2025 Jun 3;20(6):e0324974. doi: 10.1371/journal.pone.0324974. eCollection 2025. PLoS One. 2025. PMID: 40460147 Free PMC article.
-
Preservation of the PCL when performing cruciate-retaining TKA: Is the tibial tuberosity a reliable predictor of the PCL footprint location?Knee Surg Sports Traumatol Arthrosc. 2016 Jan;24(1):58-63. doi: 10.1007/s00167-014-3309-6. Epub 2014 Sep 14. Knee Surg Sports Traumatol Arthrosc. 2016. PMID: 25218577
References
-
- Becker MW, Insall JN, Faris PM. Bilateral total knee arthroplasty. One cruciate retaining and one cruciate substituting. Clin Orthop Relat Res. 1991;271:122–124. - PubMed
-
- Bolanos AA, Colizza WA, McCann PD, Gotlin RS, Wootten ME, Kahn BA, Insall JN. A comparison of isokinetic strength testing and gait analysis in patients with posterior cruciate-retaining and substituting knee arthroplasties. J Arthroplasty. 1998;13(8):906–915. doi: 10.1016/S0883-5403(98)90198-X. - DOI - PubMed
-
- Chaudhary R, Beaupre LA, Johnston DW. Knee range of motion during the first two years after use of posterior cruciate-stabilizing or posterior cruciate-retaining total knee prostheses. A randomized clinical trial. J Bone Joint Surg Am. 2008;90(12):2579–2586. doi: 10.2106/JBJS.G.00995. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
