

Impact of margin assessment method on positive margin rate and total volume excised
- PMID: 24046114
- PMCID: PMC3923624
- DOI: 10.1245/s10434-013-3257-2
Impact of margin assessment method on positive margin rate and total volume excised
Abstract
Background: For breast-conserving surgery, the method of margin assessment that most frequently achieves negative margins without increasing the volume of tissue excised is uncertain. We examined our institutional experience with three different margin assessment methods used by six experienced breast surgeons.
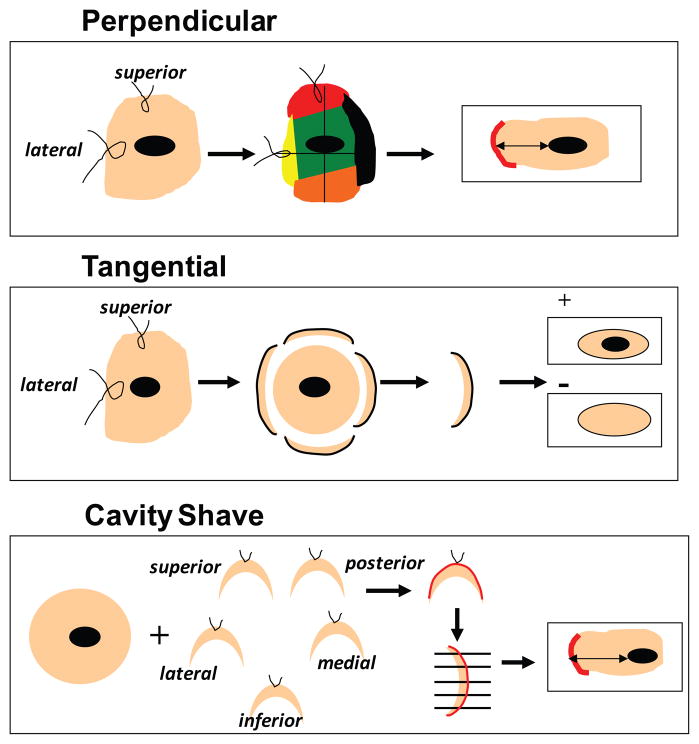
Methods: Patients undergoing breast-conserving surgery for invasive carcinoma during July to December of a representative year during which each method was performed (perpendicular, 2003; tangential, 2004; cavity shave, 2011) were included. The effect of margin method on the positive margin rate at first excision and the total volume excised to achieve negative margins were evaluated by multivariable analysis, by surgeon, and by tumor size and presence of extensive intraductal component (EIC).
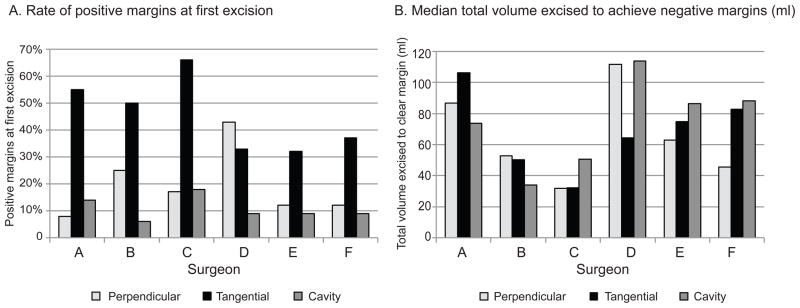
Results: A total of 555 patients were identified, as follows: perpendicular, 140; tangential, 124; and cavity shave, 291. The tangential method had a higher rate of positive margins at first excision than the perpendicular and cavity-shave methods (49, 15, 11 %, respectively; p < 0.0001). Median volumes to achieve negative margins were similar (55 ml perpendicular; 64 ml tangential; 62 ml cavity shave; p = 0.24). Four of six surgeons had the lowest rate of positive margins with the cavity-shave method, which was significant when compared to the tangential method (p < 0.0001) but not the perpendicular method (p = 0.37). The volume excised by the three methods varied by surgeon (p < 0.0001). The perpendicular method was optimal for T1 tumors without EIC; the cavity-shave method tended to be superior for T2-T3 tumors and/or EIC.
Conclusions: Although the cavity-shave method may decrease the rates of positive margins, its effect on volume is variable among surgeons and may result in an increase in the total volume excised for some surgeons and for small tumors without EIC.
Conflict of interest statement
Figures
References
-
- Showalter SL, Grover S, Sharma S, et al. Factors Influencing Surgical and Adjuvant Therapy in Stage I Breast Cancer: A SEER 18 Database Analysis. Ann Surg Oncol. 2012 - PubMed
-
- Gage I, Schnitt SJ, Nixon AJ, et al. Pathologic margin involvement and the risk of recurrence in patients treated with breast-conserving therapy. Cancer. 1996;78(9):1921–8. - PubMed
-
- Punglia RS, Morrow M, Winer EP, et al. Local therapy and survival in breast cancer. N Engl J Med. 2007;356(23):2399–405. - PubMed
-
- Kreike B, Hart AA, van de Velde T, et al. Continuing risk of ipsilateral breast relapse after breast-conserving therapy at long-term follow-up. Int J Radiat Oncol Biol Phys. 2008;71(4):1014–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
