

Variation in surgical-readmission rates and quality of hospital care
- PMID: 24047062
- PMCID: PMC4107655
- DOI: 10.1056/NEJMsa1303118
Variation in surgical-readmission rates and quality of hospital care
Abstract
Background: Reducing hospital-readmission rates is a clinical and policy priority, but little is known about variation in rates of readmission after major surgery and whether these rates at a given hospital are related to other markers of the quality of surgical care.
Methods: Using national Medicare data, we calculated 30-day readmission rates after hospitalization for coronary-artery bypass grafting, pulmonary lobectomy, endovascular repair of abdominal aortic aneurysm, open repair of abdominal aortic aneurysm, colectomy, and hip replacement. We used bivariate and multivariate techniques to assess the relationships between readmission rates and other measures of surgical quality, including adherence to surgical process measures, procedure volume, and mortality.
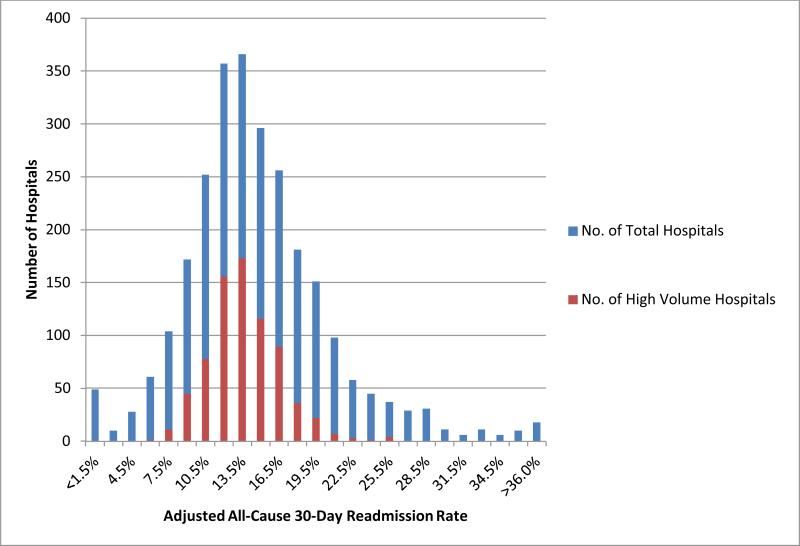
Results: For the six index procedures, there were 479,471 discharges from 3004 hospitals. The median risk-adjusted composite readmission rate at 30 days was 13.1% (interquartile range, 9.9 to 17.1). In a multivariate model adjusting for hospital characteristics, we found that hospitals in the highest quartile for surgical volume had a significantly lower composite readmission rate than hospitals in the lowest quartile (12.7% vs. 16.8%, P<0.001), and hospitals with the lowest surgical mortality rates had a significantly lower readmission rate than hospitals with the highest mortality rates (13.3% vs. 14.2%, P<0.001). High adherence to reported surgical process measures was only marginally associated with reduced readmission rates (highest quartile vs. lowest quartile, 13.1% vs. 13.6%; P=0.02). Patterns were similar when each of the six major surgical procedures was examined individually.
Conclusions: Nearly one in seven patients hospitalized for a major surgical procedure is readmitted to the hospital within 30 days after discharge. Hospitals with high surgical volume and low surgical mortality have lower rates of surgical readmission than other hospitals.
Figures
Comment in
-
Surgical-readmission rates and quality of care.N Engl J Med. 2013 Dec 19;369(25):2460-1. doi: 10.1056/NEJMc1313241. N Engl J Med. 2013. PMID: 24350963 No abstract available.
-
Surgical-readmission rates and quality of care.N Engl J Med. 2013 Dec 19;369(25):2460. doi: 10.1056/NEJMc1313241. N Engl J Med. 2013. PMID: 24350964 No abstract available.
-
Surgical-readmission rates and quality of care.N Engl J Med. 2013 Dec 19;369(25):2460. doi: 10.1056/NEJMc1313241. N Engl J Med. 2013. PMID: 24350965 No abstract available.
-
Re: variation in surgical-readmission rates and quality of hospital care.J Urol. 2014 May;191(5):1363-4. doi: 10.1016/j.juro.2014.01.050. Epub 2014 Jan 16. J Urol. 2014. PMID: 24745527 No abstract available.
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–28. - PubMed
-
- Jha AK, Orav EJ, Epstein AM. Public reporting of discharge planning and rates of readmissions. N Engl J Med. 2009;361:2637–45. - PubMed
-
- Voss R, Gardner R, Baier R, Butterfield K, Lehrman S, Gravenstein S. The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med. 2011;171:1232–7. - PubMed
-
- Readmissions Reduction Program 2012 at http://www.cms.gov/Medicare/Medicare-Feefor-Service-Payment/AcuteInpatie....)
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical