

Electrocardiographic abnormalities and elevated cTNT at admission for intracerebral hemorrhage: predictors for survival?
- PMID: 24047488
- PMCID: PMC6931947
- DOI: 10.1111/anec.12056
Electrocardiographic abnormalities and elevated cTNT at admission for intracerebral hemorrhage: predictors for survival?
Abstract
Background: Cerebrovascular lesions are often associated with electrocardiographic (ECG) abnormalities. The main purpose of this work was to investigate the prognostic value of ECG abnormalities and/or elevated cardiac troponin (cTNT) on admission in patients with nontraumatic intracerebral hemorrhage (ICH).
Methods: Ninety-seven consecutive patients with ICH were included. The predictive value of ECG abnormalities and increased TNT on survival were evaluated using Cox proportional hazard model.
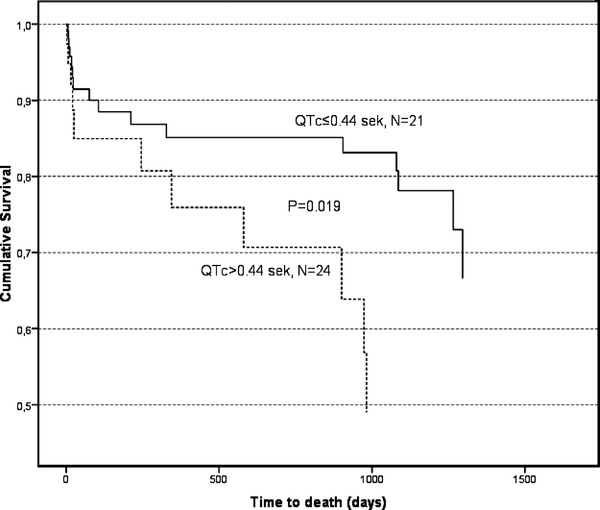
Results: The most frequently observed ECG abnormalities were the presence of a Q wave (39.6%), followed by prolonged QTc (>0.44 s; 35.4%), which was an independent predictor for long-term mortality (P = 0.019). No difference in QTc was observed between patients with right versus left ICH. Increased cTNT levels at admission had no prognostic value.
Conclusion: Various ECG changes were common in patients presenting with an ICH, but only prolonged QTc was found to be an independent predictor of poor survival during follow-up after ICH.
Keywords: ECG; QTc; cTNT; intracerebral hemorrhage; stroke prognosis.
©2013 Wiley Periodicals, Inc.
Figures
Comment in
-
Is prolonged QTc sufficient to predict survival in patients with intracerebral hemorrhage?Ann Noninvasive Electrocardiol. 2014 Mar;19(2):205-6. doi: 10.1111/anec.12142. Epub 2014 Feb 19. Ann Noninvasive Electrocardiol. 2014. PMID: 24620848 Free PMC article. No abstract available.
-
Is prolonged QTc sufficient to predict survival in patients with intracerebral hemorrhage?Ann Noninvasive Electrocardiol. 2014 Mar;19(2):203-4. doi: 10.1111/anec.12143. Epub 2014 Feb 18. Ann Noninvasive Electrocardiol. 2014. PMID: 24708272 Free PMC article. No abstract available.
Similar articles
-
Clinical importance of cardiac troponin release and cardiac abnormalities in patients with supratentorial cerebral hemorrhages.Mayo Clin Proc. 2006 Feb;81(2):192-6. doi: 10.4065/81.2.192. Mayo Clin Proc. 2006. PMID: 16471073
-
Inversion of T Waves on Admission is Associated with Mortality in Spontaneous Intracerebral Hemorrhage.J Stroke Cerebrovasc Dis. 2021 Jun;30(6):105776. doi: 10.1016/j.jstrokecerebrovasdis.2021.105776. Epub 2021 Apr 8. J Stroke Cerebrovasc Dis. 2021. PMID: 33839377
-
Prevalence and characterization of ECG abnormalities after intracerebral hemorrhage.Neurocrit Care. 2010 Feb;12(1):50-5. doi: 10.1007/s12028-009-9283-z. Neurocrit Care. 2010. PMID: 19813104
-
Prognostic value of elevated cardiac troponin I in patients with intracerebral hemorrhage.Clin Cardiol. 2020 Apr;43(4):338-345. doi: 10.1002/clc.23320. Epub 2019 Dec 18. Clin Cardiol. 2020. PMID: 31851767 Free PMC article.
-
A Narrative Review of Cardiovascular Abnormalities After Spontaneous Intracerebral Hemorrhage.J Neurosurg Anesthesiol. 2019 Apr;31(2):199-211. doi: 10.1097/ANA.0000000000000493. J Neurosurg Anesthesiol. 2019. PMID: 29389729 Review.
Cited by
-
Prognostic significance of prolonged corrected QT interval in cerebral contusion.Indian J Med Res. 2023 Aug;158(2):175-181. doi: 10.4103/ijmr.ijmr_3629_21. Indian J Med Res. 2023. PMID: 37706372 Free PMC article.
-
Serum Lactate as Serum Biomarker for Cardiopulmonary Parameters within the First 24 Hours after a Spontaneous Intracerebral Hemorrhage.Diagnostics (Basel). 2022 Oct 5;12(10):2414. doi: 10.3390/diagnostics12102414. Diagnostics (Basel). 2022. PMID: 36292103 Free PMC article.
-
Electrocardiogram alterations in non-traumatic brain injury: a systematic review.J Clin Monit Comput. 2024 Apr;38(2):407-414. doi: 10.1007/s10877-023-01075-5. Epub 2023 Sep 22. J Clin Monit Comput. 2024. PMID: 37736801
-
Serum Urea-to-Albumin Ratio Is an Independent Predictor of Intra-Hospital Mortality in Neurosurgical Intensive Care Unit Patients with Spontaneous Intracerebral Hemorrhage.J Clin Med. 2023 May 18;12(10):3538. doi: 10.3390/jcm12103538. J Clin Med. 2023. PMID: 37240644 Free PMC article.
-
Fibrinogen to Albumin Ratio as Early Serum Biomarker for Prediction of Intra-Hospital Mortality in Neurosurgical Intensive Care Unit Patients with Spontaneous Intracerebral Hemorrhage.J Clin Med. 2022 Jul 20;11(14):4214. doi: 10.3390/jcm11144214. J Clin Med. 2022. PMID: 35887976 Free PMC article.
References
-
- Juvela S. Risk factors for impaired outcome after spontaneous intracerebral hemorrhage. Arch Neurol 1995;52(12):1193–1200. - PubMed
-
- Christensen H, Fogh Christensen A, Boysen G. Abnormalities on ECG and telemetry predict stroke outcome at 3 months. J Neurol Sci 2005;234(1–2):99–103. - PubMed
-
- Randell T, Tanskanen P, Scheinin M, et al. QT dispersion after subarachnoid hemorrhage. J Neurosurg Anesthesiol 1999;11(3):163–166. - PubMed
-
- Sato K, Kato M, Yoshimoto T. QT intervals and QT dispersion in patients with subarachnoid hemorrhage. J Anesth 2001;15(2):74–77. - PubMed
-
- Golbasi Z, Selcoki Y, Eraslan T, et al. QT dispersion. Is it an independent risk factor for in‐hospital mortality in patients with intracerebral hemorrhage? Jpn Heart J 1999;40(4):405–411. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
