

One-stage combined lumbo-sacral fusion, by anterior then posterior approach: clinical and radiological results
- PMID: 24048651
- PMCID: PMC3830042
- DOI: 10.1007/s00586-013-3017-9
One-stage combined lumbo-sacral fusion, by anterior then posterior approach: clinical and radiological results
Abstract
Introduction: We intended to prospectively evaluate the clinical and radiological results of lumbo-sacral fusion achieved by a combined approach, anterior then posterior.
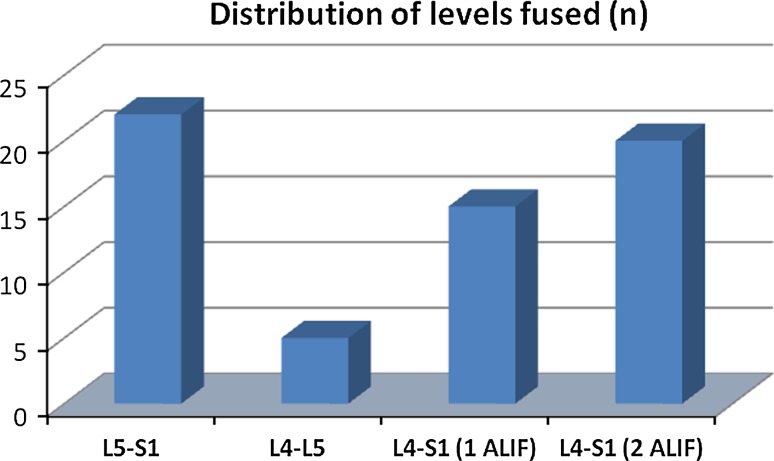
Material and methods: 62 patients were consecutively treated at L5-S1, L4-L5 or L4-S1 for degenerative disc disease or low-grade isthmic spondylolisthesis by combined surgery.
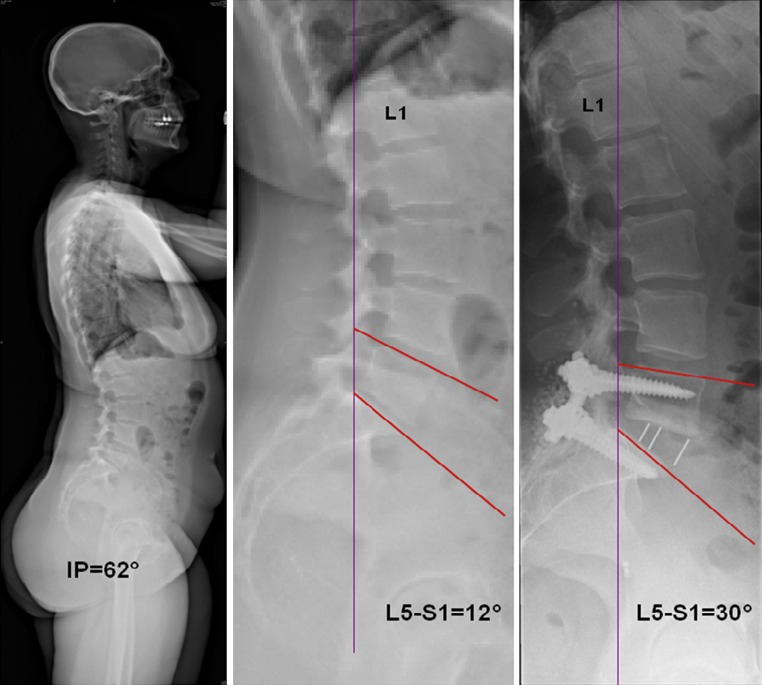
Results: Mean operative time and blood loss were 209 min and 308 ml, respectively, including the two approaches. VAS, ODI and Roland-Morris scores significantly improved postoperatively at 1 year (p < 0.005) and fusion was obtained in all cases on the CT scan at 1-year follow-up. Segmental lordosis significantly improved postoperatively (p < 0.05) with a mean gain of 10.2° at L5-S1 and 5.5° at L4-L5.
Conclusion: The combined procedure meets the requested criteria for a lumbar fusion in terms of clinical results, functional outcomes, fusion rates while restoring segmental lordosis and disc height. It cumulates the advantages of the anterior and posterior approach performed alone, especially for L5-S1.
Figures




References
-
- Athiviraham A, Yen D. Is spinal stenosis better treated surgically or nonsurgically? Clin Orthop Relat Res. 2007;458:90–93. - PubMed
-
- Kwon B, Katz JN, Kim DH, Jenis LG. A review of the 2001 Volvo award winner in clinical studies: lumbar fusion versus nonsurgical treatment for chronic low back pain: a multicenter randomized controlled trial from the Swedish lumbar spine study group. Spine (Phila Pa 1976) 2006;31(2):245–249. doi: 10.1097/01.brs.0000195346.35996.26. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
