

What is the learning curve for robotic-assisted pedicle screw placement in spine surgery?
- PMID: 24048889
- PMCID: PMC4016454
- DOI: 10.1007/s11999-013-3291-1
What is the learning curve for robotic-assisted pedicle screw placement in spine surgery?
Abstract
Background: Some early studies with robotic-assisted pedicle screw implantation have suggested these systems increase accuracy of screw placement. However, the relationship between the success rate of screw placement and the learning curve of this new technique has not been evaluated.
Questions/purposes: We determined whether, as a function of surgeon experience, (1) the success rate of robotic-assisted pedicle screw placement improved, (2) the frequency of conversion from robotic to manual screw placement decreased, and (3) the frequency of malpositioned screws decreased.
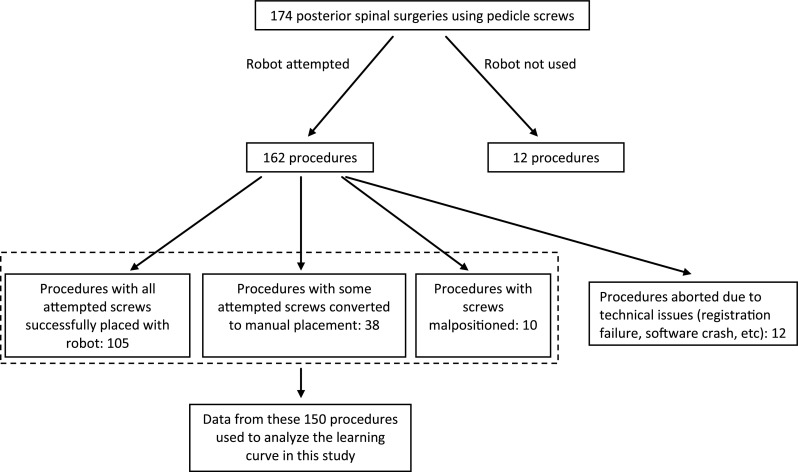
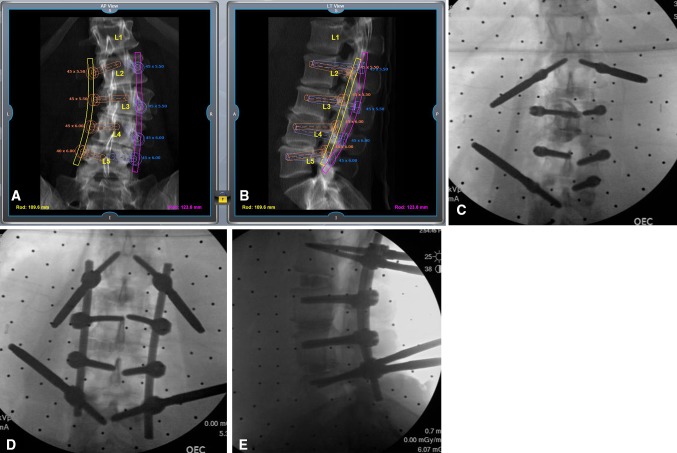
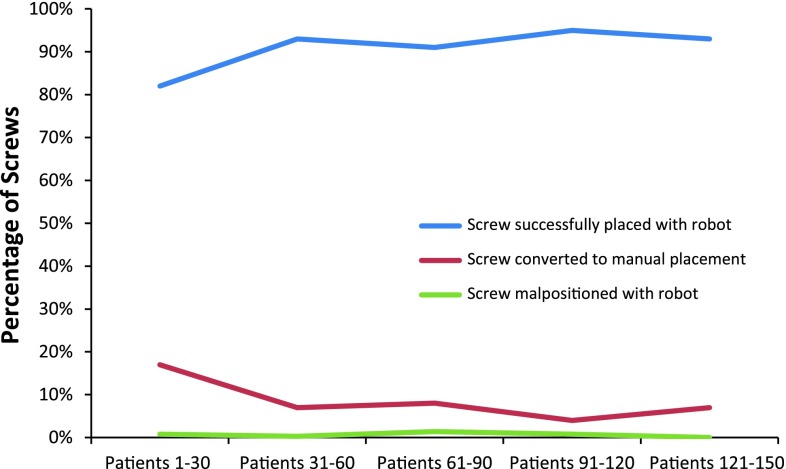
Methods: Between June 2010 and August 2012, the senior surgeon (IHL) performed 174 posterior spinal procedures using pedicle screws, 162 of which were attempted with robotic assistance. The use of the robotic system was aborted in 12 of the 162 procedures due to technical issues (registration failure, software crash, etc). The robotic system was successfully used in the remaining 150 procedures. These were the first procedures performed with the robot by the senior surgeon, and in this study, we divided the early learning curve into five groups: Group 1 (Patients 1-30), Group 2 (Patients 31-60), Group 3 (Patients 61-90), Group 4 (Patients 91-120), and Group 5 (Patients 121-150). One hundred twelve patients (75%) had spinal deformity and 80 patients (53%) had previous spine surgery. The accuracy of screw placement in the groups was assessed based on intraoperative biplanar fluoroscopy and postoperative radiographs. The results from these five groups were compared to determine the effect on the learning curve. The numbers of attempted pedicle screw placements were 359, 312, 349, 359, and 320 in Groups 1 to 5, respectively.
Results: The rates of successfully placed screws using robotic guidance were 82%, 93%, 91%, 95%, and 93% in Groups 1 to 5. The rates of screws converted to manual placement were 17%, 7%, 8%, 4%, and 7%. Of the robotically placed screws, the screw malposition rates were 0.8%, 0.3%, 1.4%, 0.8%, and 0%.
Conclusions: The rate of successfully placed pedicle screws improved with increasing experience. The rate of the screws that were converted to manual placement decreased with increasing experience. The frequency of screw malposition was similar over the learning curve at 0% to 1.4%. Future studies will need to determine whether this finding is generalizable to others.
Level of evidence: Level III, therapeutic study. See the Instructions for Authors for a complete description of levels of evidence.
Figures
References
-
- Bai YS, Zhang Y, Chen ZQ, Wang CF, Zhao YC, Shi ZC, Li M, Liu KP. Learning curve of computer-assisted navigation system in spine surgery. Chin Med J (Engl). 2010;123:2989–2994. - PubMed
-
- Devito DP, Kaplan L, Dietl R, Pfeiffer M, Horne D, Silberstein B, Hardenbrook M, Kiriyanthan G, Barzilay Y, Bruskin A, Sackerer D, Alexandrovsky V, Stuer C, Burger R, Maeurer J, Donald GD, Schoenmayr R, Friedlander A, Knoller N, Schmieder K, Pechlivanis I, Kim IS, Meyer B, Shoham M. Clinical acceptance and accuracy assessment of spinal implants guided with SpineAssist surgical robot: retrospective study. Spine (Phila Pa 1976). 2010;35:2109–2115. doi: 10.1097/BRS.0b013e3181d323ab. - DOI - PubMed
-
- Gaines RW., Jr The use of pedicle-screw internal fixation for the operative treatment of spinal disorders. J Bone Joint Surg Am. 2000;82:1458–1476. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
