Comparative analysis between 5 mm and 7.5 mm collimators in CyberKnife radiosurgery for trigeminal neuralgia
- PMID: 24049318
- PMCID: PMC3775035
- DOI: 10.4103/0971-6203.116364
Comparative analysis between 5 mm and 7.5 mm collimators in CyberKnife radiosurgery for trigeminal neuralgia
Abstract
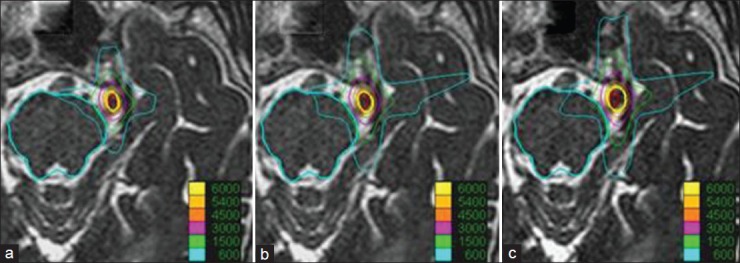
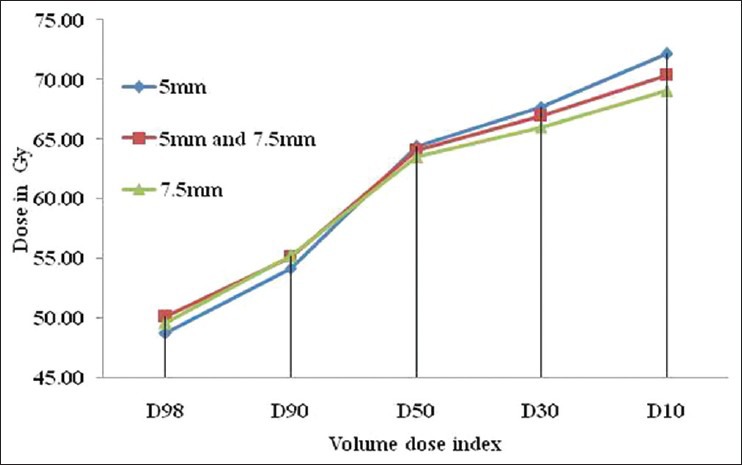
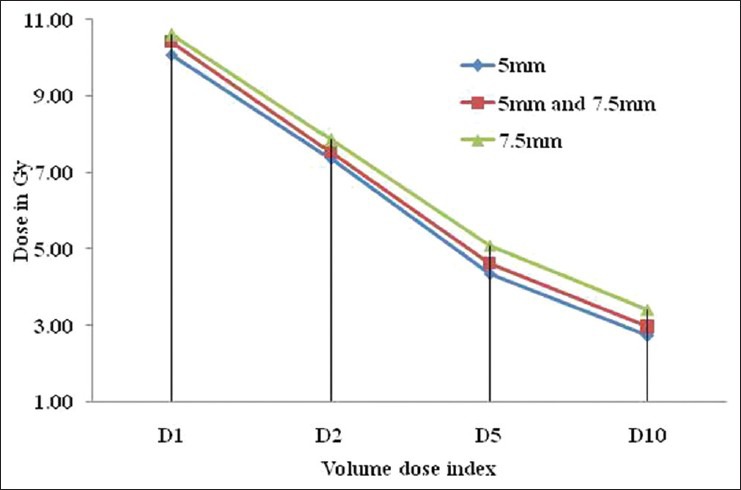
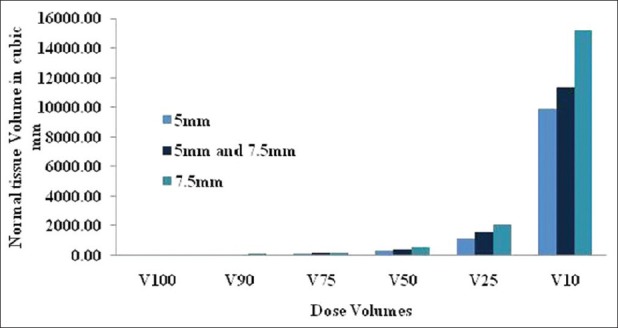
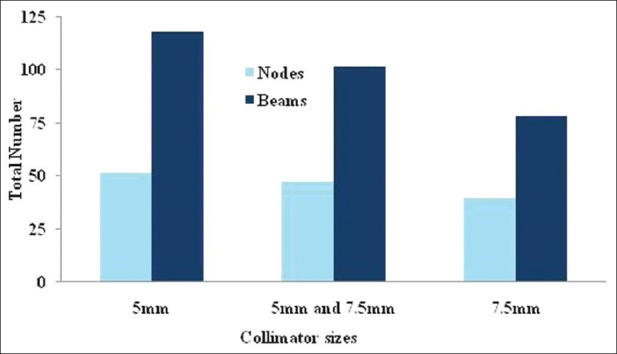
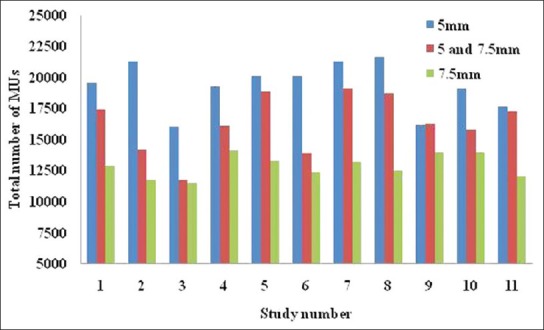
Trigeminal neuralgia (TN) is treated in CyberKnife (Accuray Inc, Sunnyvale, USA) with the 5 mm collimator whose dosimetric inaccuracy is higher than the other available collimators. The 7.5 mm collimator which is having less dosimetric uncertainty can be an alternative for 5 mm collimator provided the dose distribution with 7.5 mm collimator is acceptable. Aim of this study is to analyze the role of 7.5 mm collimator in CyberKnife treatment plans of TN. The treatment plans with 5 mm collimators were re-optimized with 7.5 mm collimator and a bi-collimator system (5 mm and 7.5 mm). The treatment plans were compared for target coverage, brainstem doses, and the dose to normal tissues. The target and brainstem doses were comparable. However, the conformity indices were 2.31 ± 0.52, 2.40 ± 0.87 and 2.82 ± 0.51 for 5 mm, bi-collimator (5mm and 7.5 mm), 7.5 mm collimator plans respectively. This shows the level of dose spillage in 7.5 mm collimator plans. The 6 Gy dose volumes in 7.5 mm plans were 1.53 and 1.34 times higher than the 5 mm plan and the bi-collimator plans respectively. The treatment time parameters were lesser for 7.5 mm collimators. Since, the normal tissue dose is pretty high in 7.5 mm collimator plans, the use of it in TN plans can be ruled out though the treatment time is lesser for these 7.5 mm collimator plans.
Keywords: Collimators; CyberKnife; stereotactic radiosurgery; trigeminal neuralgia.
Conflict of interest statement
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources