

Considering Apical Scotomas, Confusion, and Diplopia When Prescribing Prisms for Homonymous Hemianopia
- PMID: 24049719
- PMCID: PMC3763894
- DOI: 10.1167/tvst.2.4.2
Considering Apical Scotomas, Confusion, and Diplopia When Prescribing Prisms for Homonymous Hemianopia
Abstract
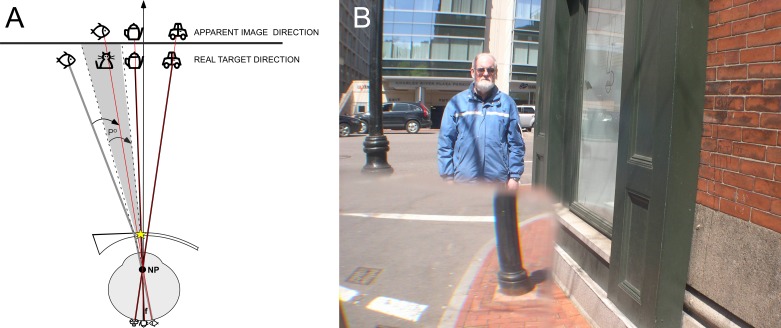
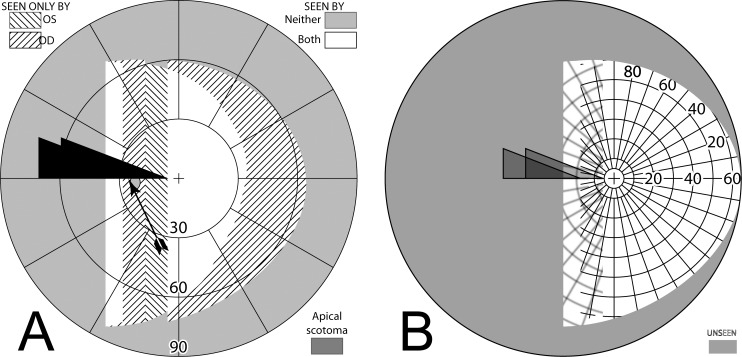
Purpose: While prisms are commonly prescribed for homonymous hemianopia to extend or expand the visual field, they cause potentially troubling visual side effects, including nonveridical location of perceived images, diplopia, and visual confusion. In addition, the field behind a prism at its apex is lost to an apical scotoma equal in magnitude to the amount of prism shift. The perceptual consequences of apical scotomas and the other effects of various designs were examined to consider parameters and designs that can mitigate the impact of these effects.
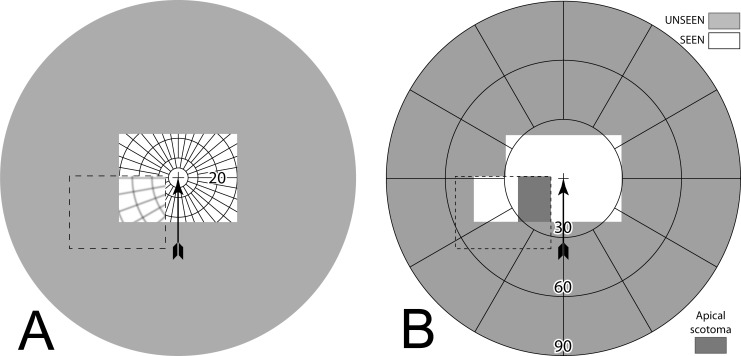
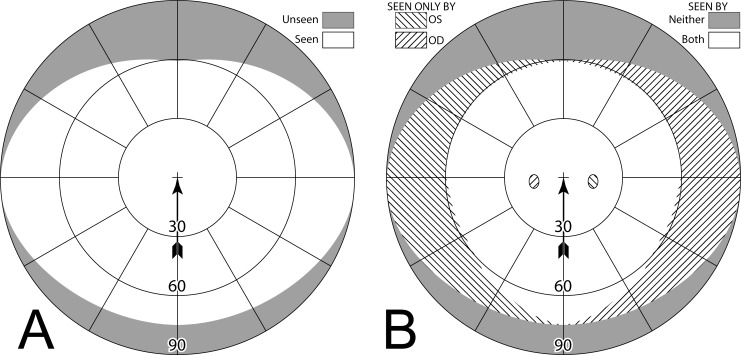
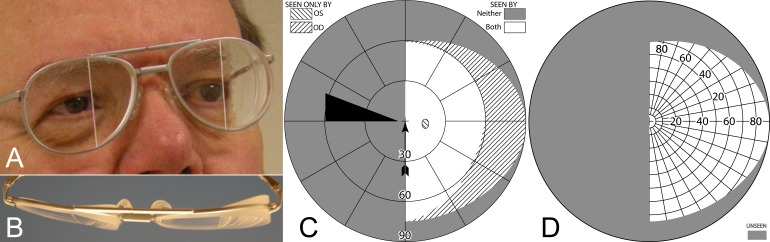
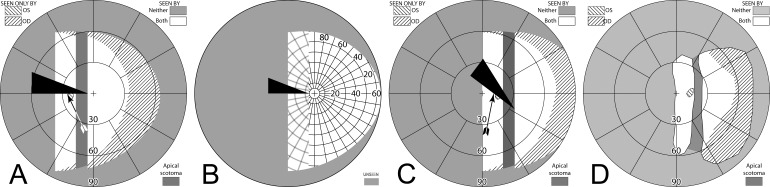
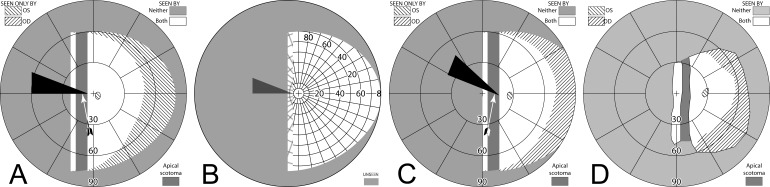
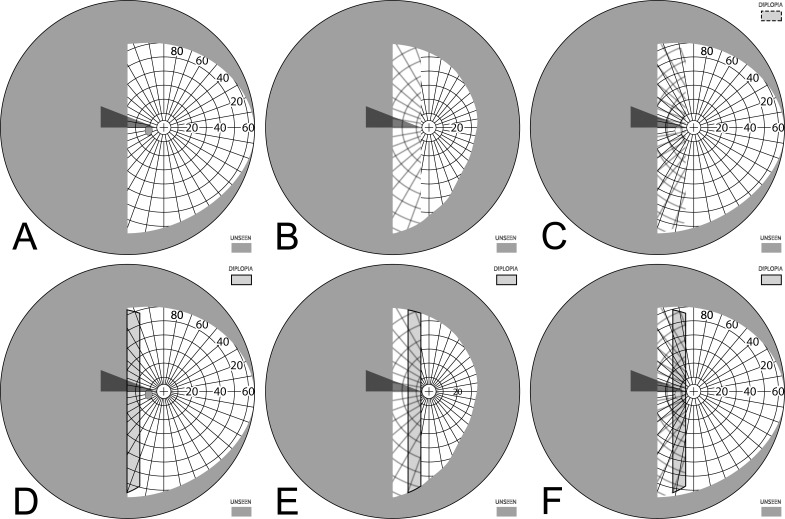
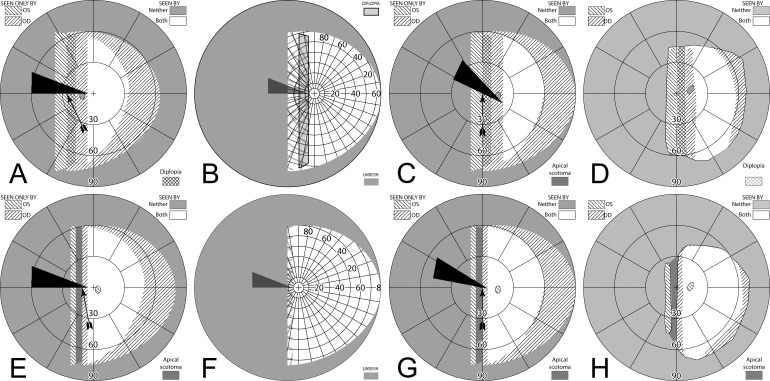
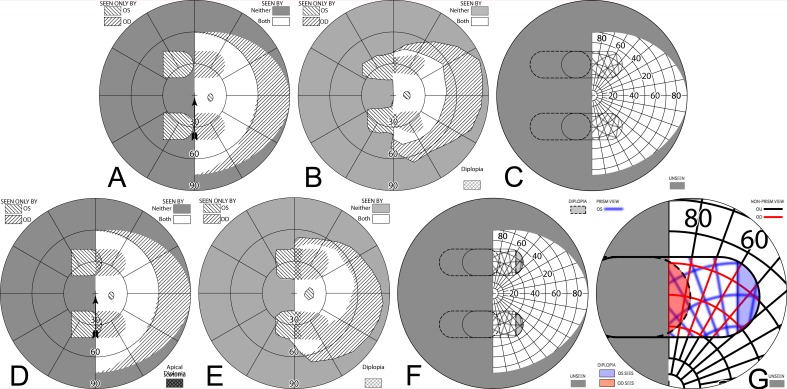
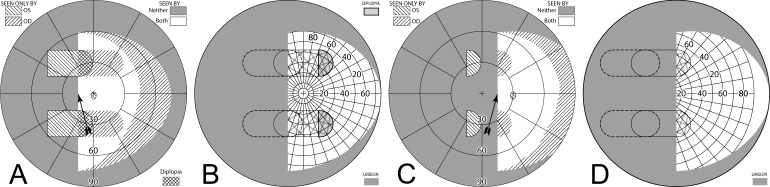
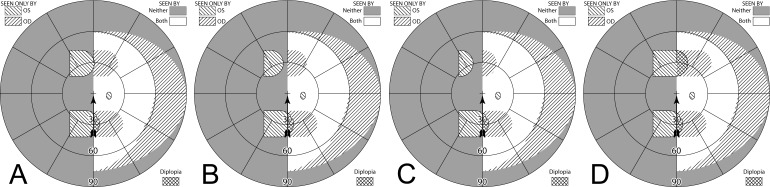
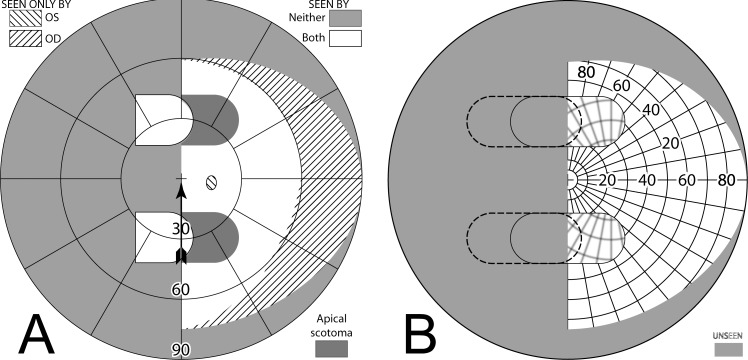
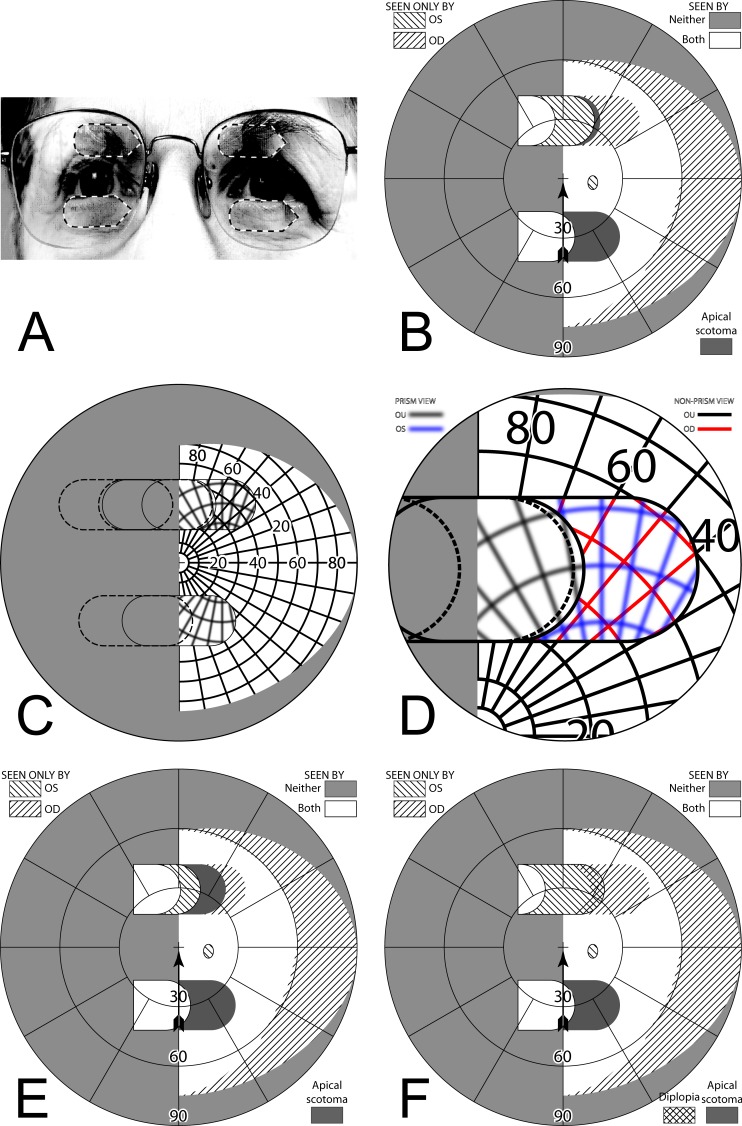
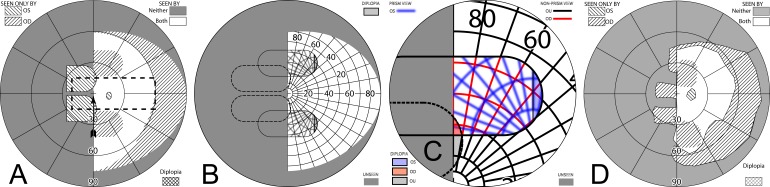
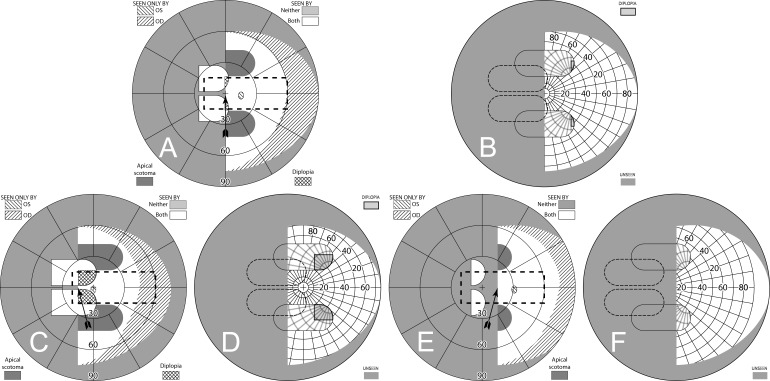
Methods: Various configurations of sector and peripheral prisms were analyzed, in various directions of gaze, and their visual effects were illustrated using simulated perimetry. A novel "percept" diagram was developed that yielded insights into the patient's view through the prisms. The predictions were verified perimetrically with patients.
Results: The diagrams distinguish between potentially beneficial field expansion via visual confusion and the pericentrally disturbing and useless effect of diplopia, and their relationship to prism power and gaze direction. They also illustrate the nonexpanding substitution of field segments of some popular prism designs.
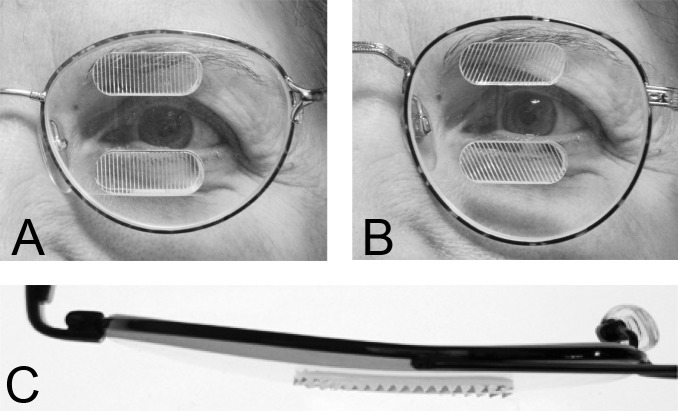
Conclusions: Yoked sector prisms have no effect at primary gaze or when gaze is directed toward the seeing hemifield, and they introduce pericentral field loss when gaze is shifted into them. When fitted unilaterally, sector prisms also have an effect only when the gaze is directed into the prism and may cause a pericentral scotoma and/or central diplopia. Peripheral prisms are effective at essentially all gaze angles. Since gaze is not directed into them, they avoid problematic pericentral effects. We derive useful recommendations for prism power and position parameters, including novel ways of fitting prisms asymmetrically.
Translational relevance: Clinicians will find these novel diagrams, diagramming techniques, and analyses valuable when prescribing prismatic aids for hemianopia and when designing new prism devices for patients with various types of field loss.
Keywords: TBI; hemianopia; low vision; perimetry; prism treatment; rehabilitation; stroke; traumatic brain injury; visual field loss.
Figures
References
-
- Zhang X, Kedar S, Lynn MJ, Newman NJ, Biousse V. Natural history of homonymous hemianopia. Neurology. 2006;66:901–905. - PubMed
-
- Papageorgiou E, Hardiess G, Schaeffel F, et al. Assessment of vision-related quality of life in patients with homonymous visual field defects. Graefe's Arch Clin Exp Ophthalmol. 2007;245:1749–1758. - PubMed
-
- Dickinson C. Low Vision: Principles and Practice. Oxford, England: Butterworth;; 1998. pp. 189–190.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
