

Patient choice in the selection of hospitals by 9-1-1 emergency medical services providers in trauma systems
- PMID: 24050797
- PMCID: PMC3785298
- DOI: 10.1111/acem.12213
Patient choice in the selection of hospitals by 9-1-1 emergency medical services providers in trauma systems
Abstract
Objectives: Reasons for undertriage (transporting seriously injured patients to nontrauma centers) and the apparent lack of benefit of trauma centers among older adults remain unclear; understanding emergency medical services (EMS) provider reasons for selecting certain hospitals in trauma systems may provide insight to these issues. In this study, the authors evaluated reasons cited by EMS providers for selecting specific hospital destinations for injured patients, stratified by age, injury severity, field triage status, and prognosis.
Methods: This was a retrospective cohort study of injured children and adults transported by 61 EMS agencies to 93 hospitals (trauma and nontrauma centers) in five regions of the western United States from 2006 through 2008. Hospital records were probabilistically linked to EMS records using trauma registries, state discharge data, and emergency department data. The seven standardized reasons cited by EMS providers for selecting hospital destinations included closest facility, ambulance diversion, physician choice, law enforcement choice, patient or family choice, specialty resource center, and other. "Serious injury" was defined as an Injury Severity Score (ISS) ≥ 16, and unadjusted in-hospital mortality was considered as a marker of prognosis. All analyses were stratified by age in 10-year increments, and descriptive statistics were used to characterize the findings.
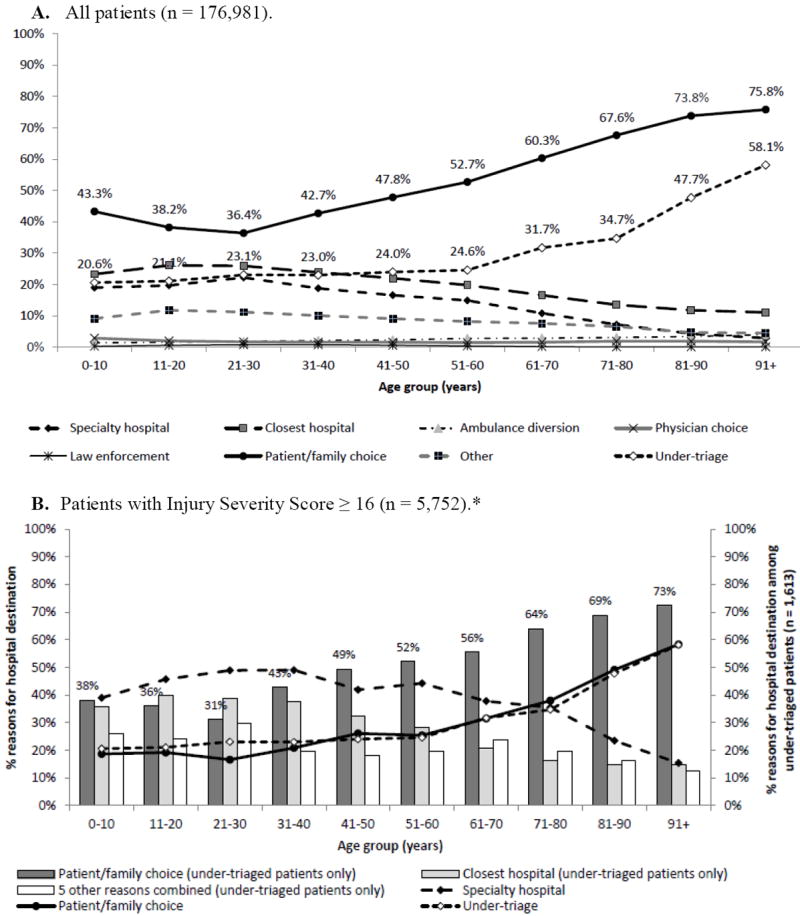
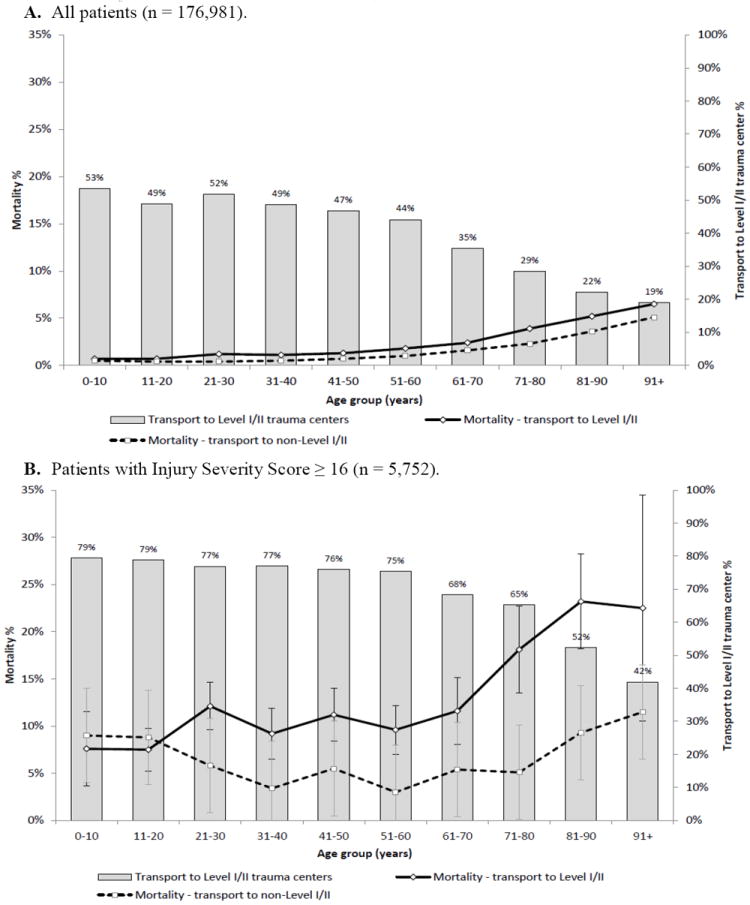
Results: A total of 176,981 injured patients were evaluated and transported by EMS over the 3-year period, of whom 5,752 (3.3%) had ISS ≥ 16 and 2,773 (1.6%) died. Patient or family choice (50.6%), closest facility (20.7%), and specialty resource center (15.2%) were the most common reasons indicated by EMS providers for selecting destination hospitals; these frequencies varied substantially by patient age. The frequency of patient or family choice increased with increasing age, from 36.4% among 21- to 30-year-olds to 75.8% among those older than 90 years. This trend paralleled undertriage rates and persisted when restricted to patients with serious injuries. Older patients with the worst prognoses were preferentially transported to major trauma centers, a finding that was not explained by field triage protocols.
Conclusions: Emergency medical services transport patterns among injured patients are not random, even after accounting for field triage protocols. The selection of hospitals appears to be heavily influenced by patient or family choice, which increases with patient age and involves inherent differences in patient prognosis.
© 2013 by the Society for Academic Emergency Medicine.
Figures
Comment in
-
Patient-centered regionalization: including the patient voice in hospital selection for time-critical illness.Acad Emerg Med. 2014 Feb;21(2):214-6. doi: 10.1111/acem.12295. Epub 2014 Jan 7. Acad Emerg Med. 2014. PMID: 24397581 No abstract available.
References
-
- Mackersie RC. History of trauma field triage development and the American College of Surgeons criteria. Prehosp Emerg Care. 2006;10:287–94. - PubMed
-
- American College of Surgeons. Resources for the Optimal Care of the Injured Patient. Chicago, IL: American College of Surgeons; 2006.
-
- Centers for Disease Control and Prevention. Guidelines for field triage of injured patients: recommendations of the national expert panel on field triage. MMWR Morbid Mortal Wkly Rep. 2009;58:1–35. - PubMed
-
- Vassar MJ, Holcroft JJ, Knudson MM, Kizer KW. Fractures in access to and assessment of trauma systems. J Am Coll Surg. 2003;197:717–25. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
