

Characterising the complexity of medication safety using a human factors approach: an observational study in two intensive care units
- PMID: 24050986
- PMCID: PMC3938094
- DOI: 10.1136/bmjqs-2013-001828
Characterising the complexity of medication safety using a human factors approach: an observational study in two intensive care units
Abstract
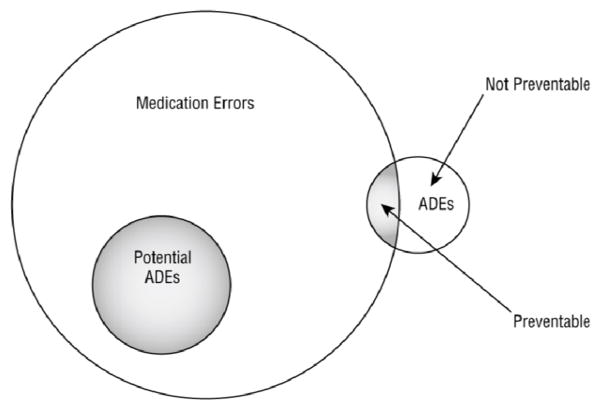
Objective: To examine medication safety in two intensive care units (ICU), and to assess the complexity of medication errors and adverse drug events (ADE) in ICUs across the stages of the medication-management process.
Methods: Four trained nurse data collectors gathered data on medication errors and ADEs between October 2006 and March 2007. Patient care documents (eg, medication order sheets, notes) and incident reports were used to identify medication errors and ADEs in a 24-bed adult medical/surgical ICU and an 18-bed cardiac ICU in a tertiary care, community teaching hospital. In this cross-sectional study, a total of 630 consecutive ICU patient admissions were assessed to produce data on the number, rates and types of potential and preventable ADEs across stages of the medication-management process.
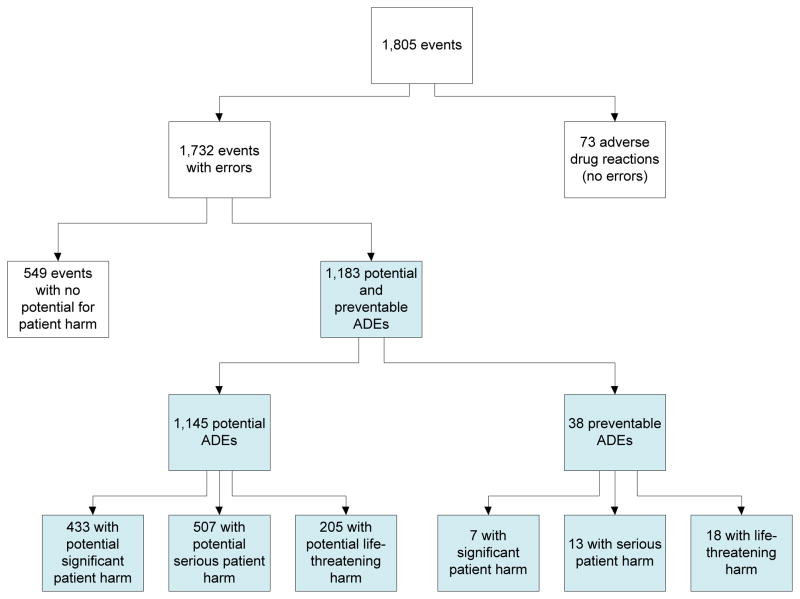
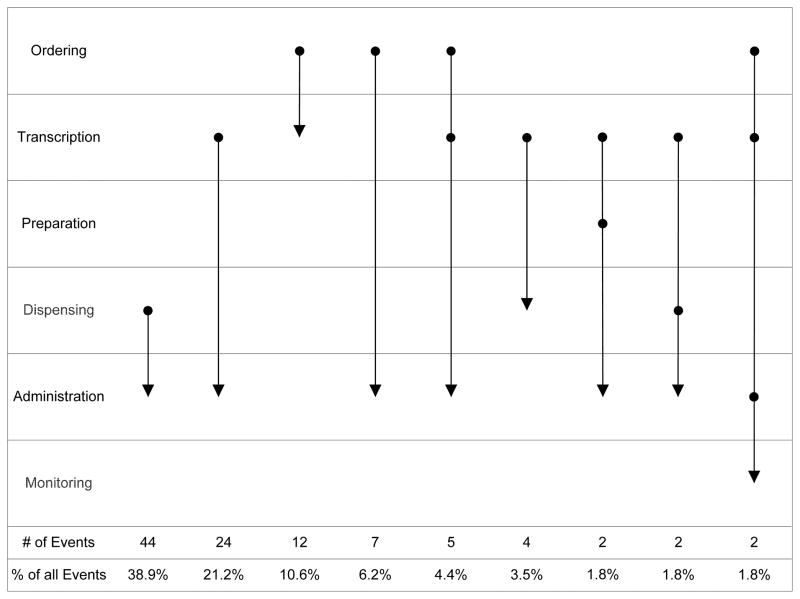
Results: An average of 2.9 preventable or potential ADEs occurred in each admission, that is, 0.4 events per patient-day. Preventable or potential ADEs occurred in 2.6% of the medication orders. The rate of potential ADEs per 1000 patient-days was 276, whereas the rate of preventable ADEs per 1000 patient-days was 9.2. Most medication errors occur at the ordering (32%) and administration stages (39%). In 16-24% of potential and preventable ADEs, clusters of errors occurred either as a sequence of errors (eg, delay in medication dispensing leading to delay in medication administration) or grouped errors (eg, route and frequency errors in the order for a medication). Many of the sequences led to administration errors that were caused by errors earlier in the medication-management process.
Conclusions: Understanding the complexity of the vulnerabilities of the medication-management process is important to devise solutions to improve patient safety. Electronic health record technology with computerised physician order entry may be one step necessary to improve medication safety in ICUs. Solutions that target multiple stages of the medication-management process are necessary to address sequential errors.
Keywords: Critical Care; Human Factors; Medication Safety.
Conflict of interest statement
Conflict of interest disclosures: No conflict of interest.
Figures
Comment in
-
Medication errors: do they occur in isolation?BMJ Qual Saf. 2014 May;23(5):e1. doi: 10.1136/bmjqs-2014-002924. Epub 2014 Feb 27. BMJ Qual Saf. 2014. PMID: 24578524 No abstract available.
References
-
- Rothschild JM, Landrigan CP, Cronin JW, et al. The Critical Care Safety Study: The incidence and nature of adverse events and serious medical errors in intensive care. Crit Care Med. 2005;33:1694–700. - PubMed
-
- Cullen DJ, Sweitzer BJ, Bates DW, et al. Preventable adverse drug events in hospitalized patients: A comparative study of intensive care and general care units. Crit Care Med. 1997;25(8):1289–97. - PubMed
-
- Harris CB, Krauss MJ, Coopersmith CM, et al. Patient safety event reporting in critical care: a study of three intensive care units. Crit Care Med. 2007;35(4):1068–76. - PubMed
-
- Bates DW, Leape LL, Cullen DJ, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998;280(15):1311–16. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical