

CVID-associated TACI mutations affect autoreactive B cell selection and activation
- PMID: 24051380
- PMCID: PMC3786721
- DOI: 10.1172/JCI69854
CVID-associated TACI mutations affect autoreactive B cell selection and activation
Abstract
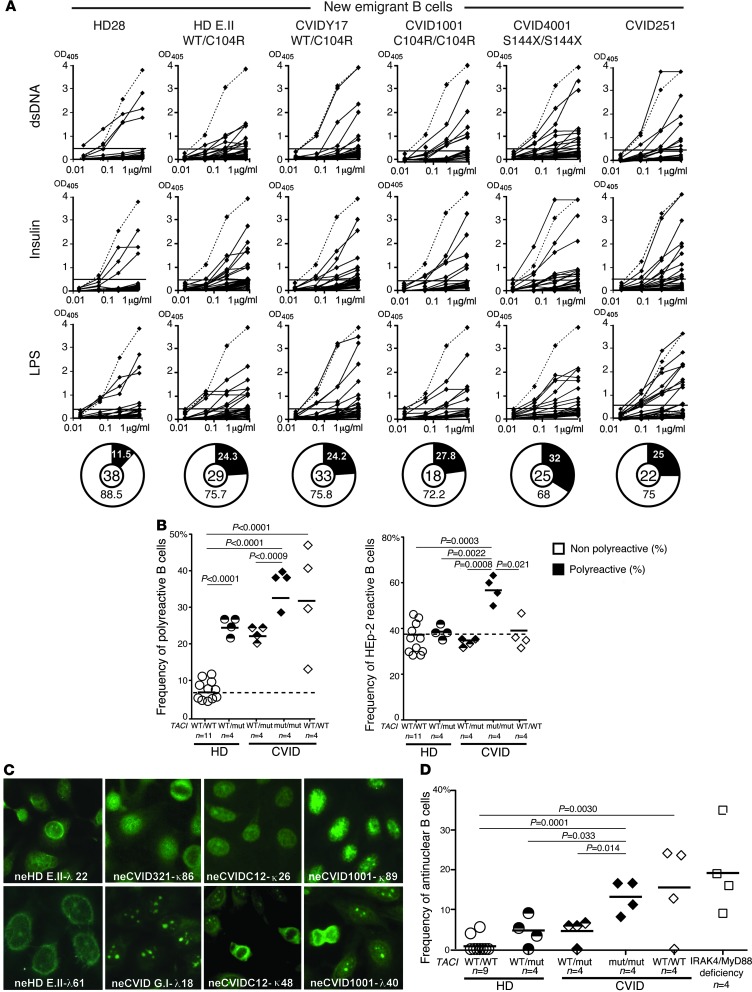
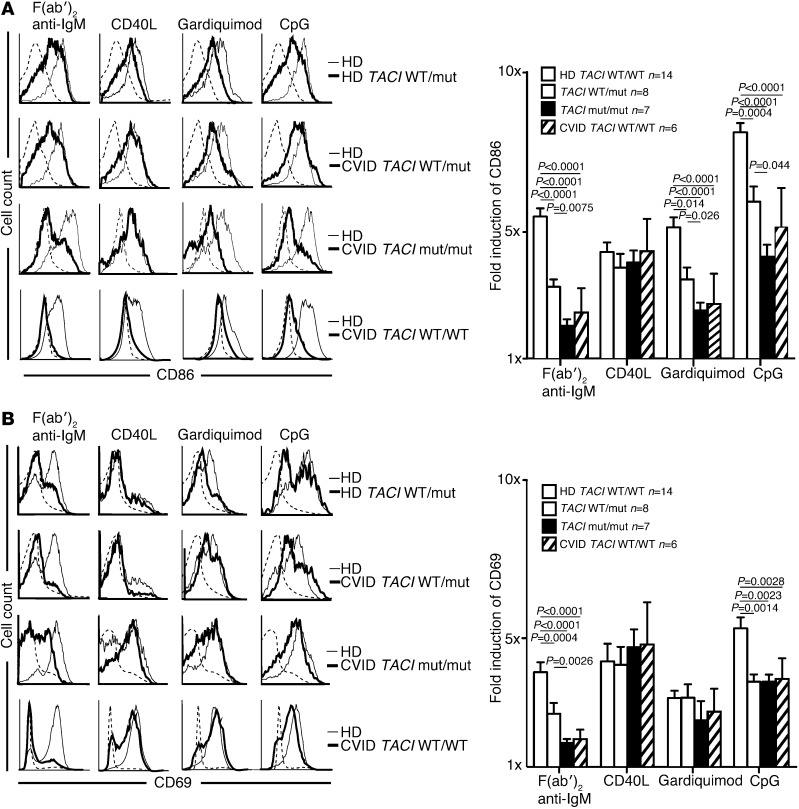
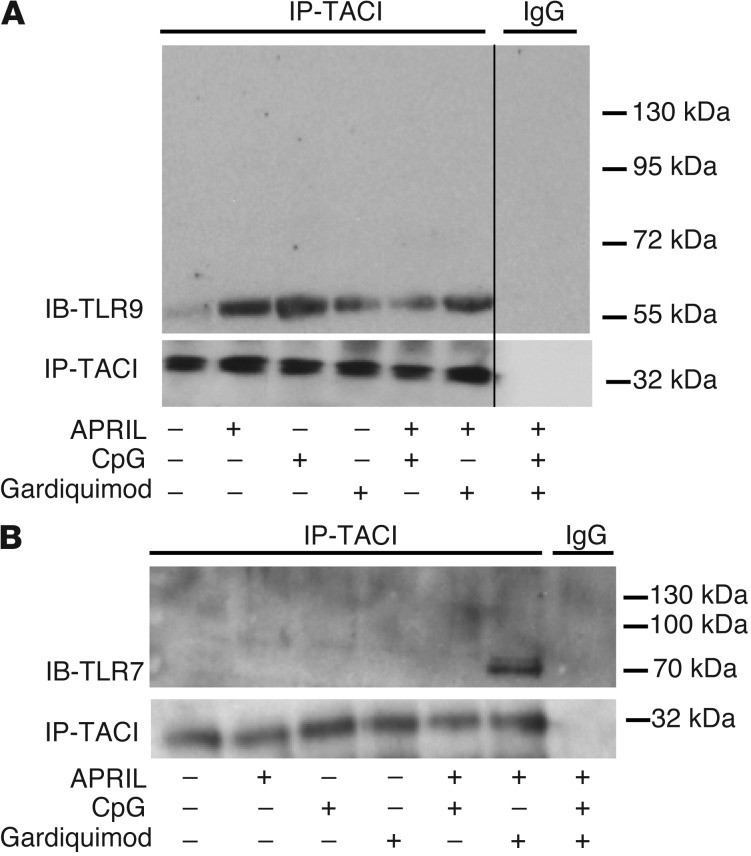
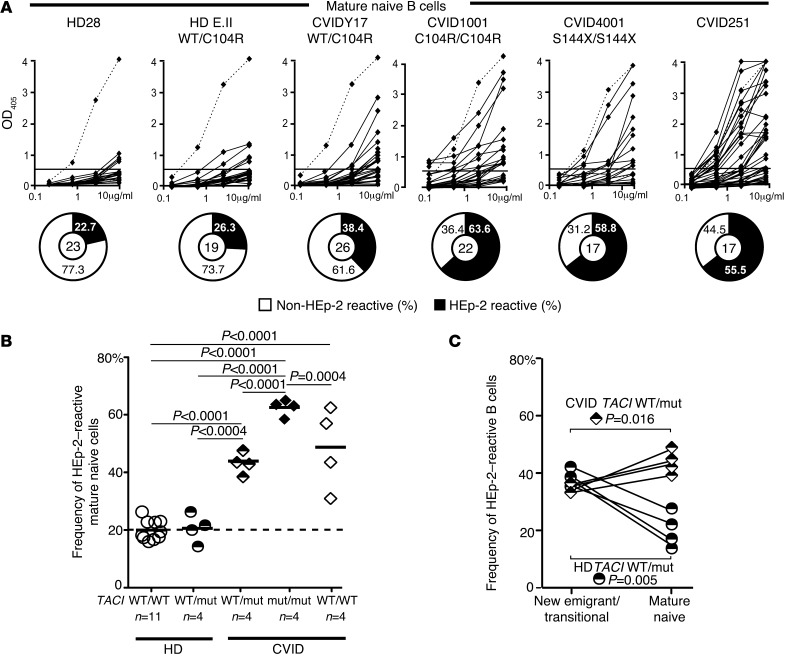
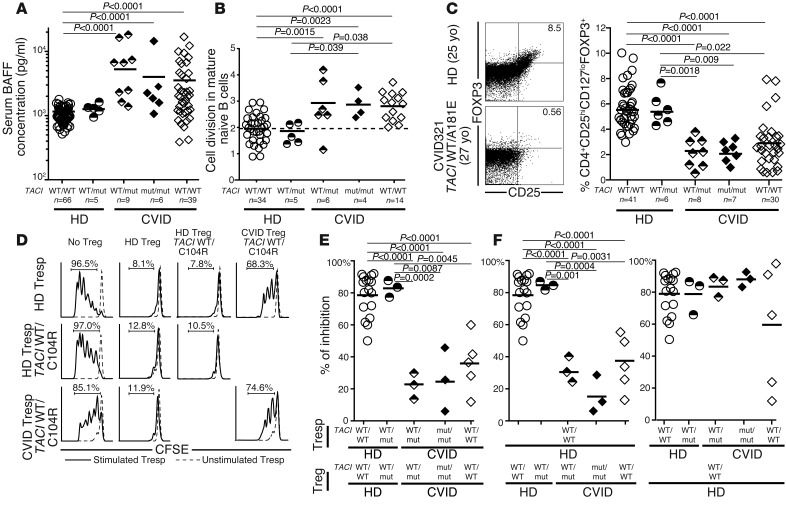
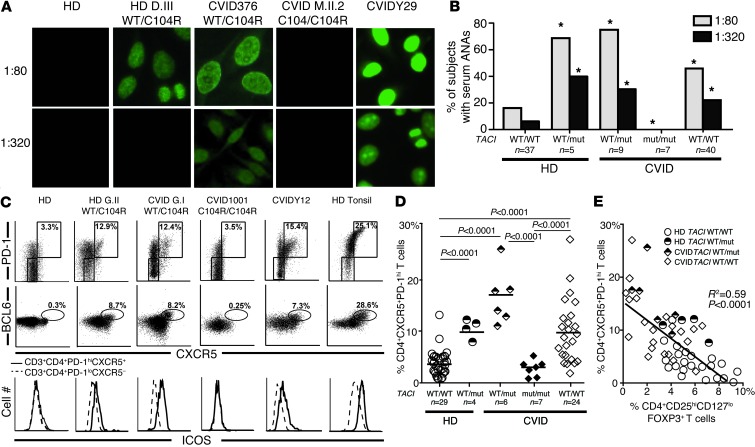
Common variable immune deficiency (CVID) is an assorted group of primary diseases that clinically manifest with antibody deficiency, infection susceptibility, and autoimmunity. Heterozygous mutations in the gene encoding the tumor necrosis factor receptor superfamily member TACI are associated with CVID and autoimmune manifestations, whereas two mutated alleles prevent autoimmunity. To assess how the number of TACI mutations affects B cell activation and tolerance checkpoints, we analyzed healthy individuals and CVID patients carrying one or two TACI mutations. We found that TACI interacts with the cleaved, mature forms of TLR7 and TLR9 and plays an important role during B cell activation and the central removal of autoreactive B cells in healthy donors and CVID patients. However, only subjects with a single TACI mutation displayed a breached immune tolerance and secreted antinuclear antibodies (ANAs). These antibodies were associated with the presence of circulating B cell lymphoma 6-expressing T follicular helper (Tfh) cells, likely stimulating autoreactive B cells. Thus, TACI mutations may favor CVID by altering B cell activation with coincident impairment of central B cell tolerance, whereas residual B cell responsiveness in patients with one, but not two, TACI mutations enables autoimmune complications.
Figures
Comment in
-
Common variable immunodeficiency: two mutations are better than one.J Clin Invest. 2013 Oct;123(10):4142-3. doi: 10.1172/JCI72476. Epub 2013 Sep 24. J Clin Invest. 2013. PMID: 24051372 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
- AI095848/AI/NIAID NIH HHS/United States
- R01 AI071087/AI/NIAID NIH HHS/United States
- AI071087/AI/NIAID NIH HHS/United States
- P01 AI061093/AI/NIAID NIH HHS/United States
- AI082713/AI/NIAID NIH HHS/United States
- U19 AI082713/AI/NIAID NIH HHS/United States
- T32 AI089704/AI/NIAID NIH HHS/United States
- R21 AI095848/AI/NIAID NIH HHS/United States
- U19 AI096187/AI/NIAID NIH HHS/United States
- R01 AI057653/AI/NIAID NIH HHS/United States
- AI061093/AI/NIAID NIH HHS/United States
- K12HD0141401-10/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
