

Surgical specimens, haemodynamics and long-term outcomes after pulmonary endarterectomy
- PMID: 24052543
- PMCID: PMC3913220
- DOI: 10.1136/thoraxjnl-2013-203746
Surgical specimens, haemodynamics and long-term outcomes after pulmonary endarterectomy
Abstract
Background: Chronic thromboembolic pulmonary hypertension is surgically curable by pulmonary endarterectomy (PEA). It is unclear whether PEA impacts primarily steady state right ventricular afterload (ie, pulmonary vascular resistance (PVR)) or pulsatile right ventricular afterload (ie, pulmonary arterial compliance (C(PA))). Our objectives were to (1) quantify PEA specimens and measure the impact of PEA on PVR and C(PA) in a structure/function study and (2) analyse the effects of haemodynamic changes on long-term survival/freedom of lung transplantation in an outcome study.
Methods: Thrombi were laid out, weighed, photographed and measured. PVR, C(PA) and resistance times compliance (RC-time) were assessed at baseline, within 4 days after PEA ('immediately postoperative') and 1 year after PEA, in 110 consecutive patients who were followed for 34.5 (11.9; 78.3) months.
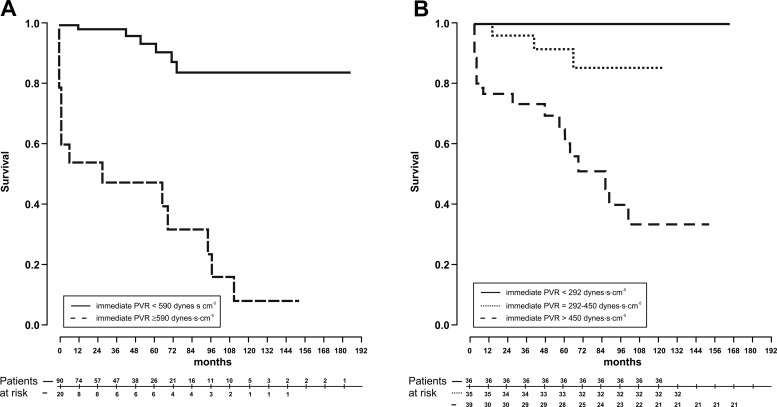
Results: Lengths and numbers of PEA specimen tails were inversely correlated with immediate postoperative PVR (p<0.0001, r=-0.566; p<0.0001, r=-0.580). PVR and C(PA) normalised immediately postoperatively while RC-time remained unchanged. Immediate postoperative PVR was the only predictor of long-term survival/freedom of lung transplantation (p<0.0001). Patients with immediate postoperative PVR<590 dynes.s.cm(-5) had better long-term outcomes than patients with PVR≥590 dynes.s.cm(-5) (p<0.0001, respectively).
Conclusions: PEA immediately decreased PVR and increased C(PA) under a constant RC-time. However, immediate postoperative PVR was the only predictor of long-term survival/freedom of lung transplantation. Our study confirms the importance of a complete, bilateral surgical endarterectomy. Low PVR measured immediately postoperative predicts excellent long-term outcome.
Keywords: Primary Pulmonary Hypertension; Pulmonary Embolism.
Figures





References
-
- Jamieson SW, Kapelanski DP, Sakakibara N, et al. Pulmonary endarterectomy: experience and lessons learned in 1,500 cases. Ann Thorac Surg 2003;76:1457–62; discussion 1462–1454 - PubMed
-
- Mayer E, Jenkins D, Lindner J, et al. Surgical management and outcome of patients with chronic thromboembolic pulmonary hypertension: results from an international prospective registry. J Thorac Cardiovasc Surg 2011;141:702–10 - PubMed
-
- Thistlethwaite PA, Kaneko K, Madani MM, et al. Technique and outcomes of pulmonary endarterectomy surgery. Ann Thorac Cardiovasc Surg 2008;14:274–82 - PubMed
-
- Madani MM, Auger WR, Pretorius V, et al. Pulmonary endarterectomy: recent changes in a single institution's experience of more than 2,700 patients. Ann Thorac Surg 2012;94:97–103;discussion 103 - PubMed
-
- Stevens GR, Garcia-Alvarez A, Sahni S, et al. RV dysfunction in pulmonary hypertension is independently related to pulmonary artery stiffness. JACC Cardiovasc Imaging 2012;5:378–87 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials