

Assessing malaria transmission in a low endemicity area of north-western Peru
- PMID: 24053144
- PMCID: PMC3849384
- DOI: 10.1186/1475-2875-12-339
Assessing malaria transmission in a low endemicity area of north-western Peru
Abstract
Background: Where malaria endemicity is low, control programmes need increasingly sensitive tools for monitoring malaria transmission intensity (MTI) and to better define health priorities. A cross-sectional survey was conducted in a low endemicity area of the Peruvian north-western coast to assess the MTI using both molecular and serological tools.
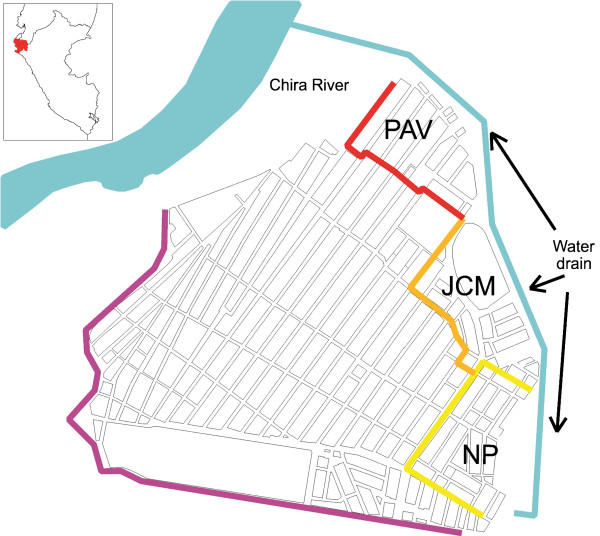
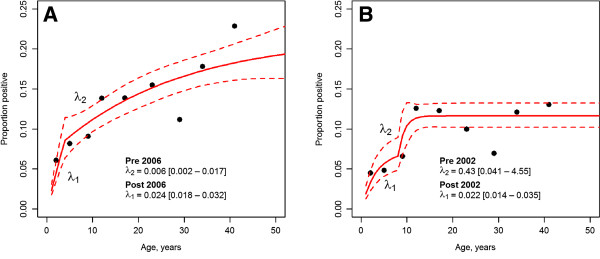
Methods: Epidemiological, parasitological and serological data were collected from 2,667 individuals in three settlements of Bellavista district, in May 2010. Parasite infection was detected using microscopy and polymerase chain reaction (PCR). Antibodies to Plasmodium vivax merozoite surface protein-119 (PvMSP1₁₉) and to Plasmodium falciparum glutamate-rich protein (PfGLURP) were detected by ELISA. Risk factors for exposure to malaria (seropositivity) were assessed by multivariate survey logistic regression models. Age-specific antibody prevalence of both P. falciparum and P. vivax were analysed using a previously published catalytic conversion model based on maximum likelihood for generating seroconversion rates (SCR).
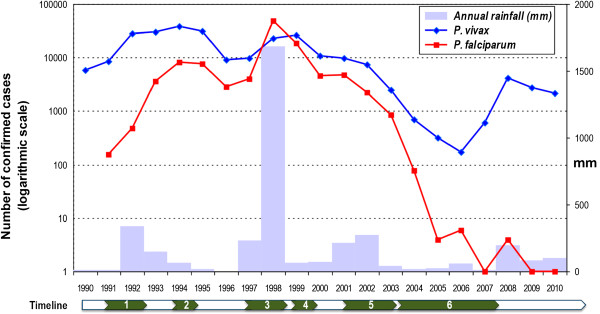
Results: The overall parasite prevalence by microscopy and PCR were extremely low: 0.3 and 0.9%, respectively for P. vivax, and 0 and 0.04%, respectively for P. falciparum, while seroprevalence was much higher, 13.6% for P. vivax and 9.8% for P. falciparum. Settlement, age and occupation as moto-taxi driver during previous year were significantly associated with P. falciparum exposure, while age and distance to the water drain were associated with P. vivax exposure. Likelihood ratio tests supported age seroprevalence curves with two SCR for both P. vivax and P. falciparum indicating significant changes in the MTI over time. The SCR for PfGLURP was 19-fold lower after 2002 as compared to before (λ1 = 0.022 versus λ2 = 0.431), and the SCR for PvMSP1₁₉ was four-fold higher after 2006 as compared to before (λ1 = 0.024 versus λ2 = 0.006).
Conclusion: Combining molecular and serological tools considerably enhanced the capacity of detecting current and past exposure to malaria infections and related risks factors in this very low endemicity area. This allowed for an improved characterization of the current human reservoir of infections, largely hidden and heterogeneous, as well as providing insights into recent changes in species specific MTIs. This approach will be of key importance for evaluating and monitoring future malaria elimination strategies.
Figures
References
-
- WHO Global Malaria Programme. World malaria report 2011. Geneva: WHO; 2011.
-
- Marquiño W, MacArthur JR, Barat LM, Oblitas FE, Arrunátegui M, Garavito G, Chafloque ML, Pardavé B, Gutierrez S, Arróspide N, Carrillo C, Cabezas C, Ruebush TK 2nd. Efficacy of chloroquine, sulfadoxine-pyrimethamine, and mefloquine for the treatment of uncomplicated Plasmodium falciparum malaria on the north coast of Peru. Am J Trop Med Hyg. 2003;68:120–123. - PubMed
-
- Marquiño W, Huilca M, Calampa C, Falconí E, Cabezas C, Naupay R, Ruebush TK 2nd. Efficacy of mefloquine and a mefloquine-artesunate combination therapy for the treatment of uncomplicated Plasmodium falciparum malaria in the Amazon Basin of Peru. Am J Trop Med Hyg. 2003;68:608–612. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
