

Mixed venous O2 saturation and fluid responsiveness after cardiac or major vascular surgery
- PMID: 24053433
- PMCID: PMC3848814
- DOI: 10.1186/1749-8090-8-189
Mixed venous O2 saturation and fluid responsiveness after cardiac or major vascular surgery
Abstract
Background: It is unclear if and how SvO2 can serve as an indicator of fluid responsiveness in patients after cardiac or major vascular surgery.
Methods: This was a substudy of a randomized single-blinded clinical trial reported earlier on critically ill patients with clinical hypovolemia after cardiac or major vascular surgery. Colloid fluid loading was done for 90 min, guided by changes in pulmonary artery occlusion pressure (PAOP) or central venous pressure (CVP). Fluid responsiveness was defined as ≥15% increase in cardiac index (CI). Hemodynamics, including transpulmonary dilution-derived global end-diastolic volume index (GEDVI) and global ejection fraction (GEF), were measured and blood samples taken.
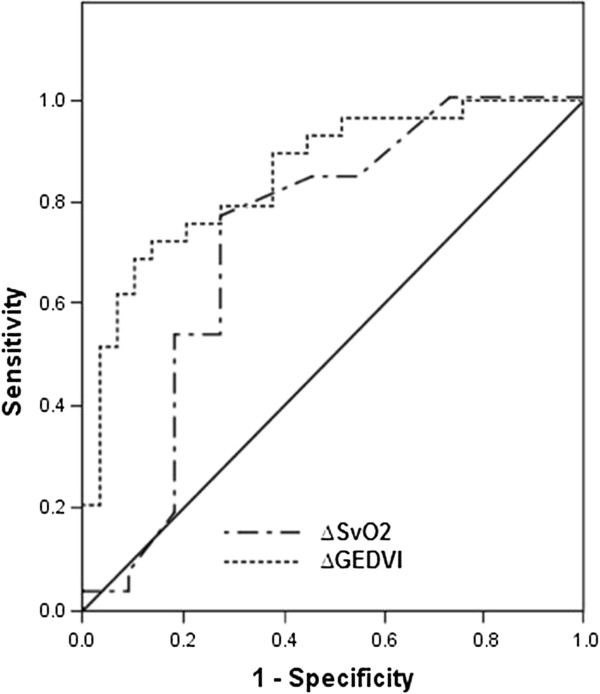
Results: Whereas baseline SvO2 (>70% in 68% of patients) did not differ, the SvO2 increased in patients responding to fluid loading (≥15% in CI in n = 26) versus those not responding (n = 11; P = 0.03). The increase in GEDVI was also greater in responders (P = 0.005). The area under the receiver operating characteristic curve for fluid responsiveness of changes in SvO2 was 0.73 (P = 0.007), with an optimal cutoff of 2%, and of those in GEDVI 0.82 (P < 0.001), while the areas did not differ. However, the value of SvO2 increases to reflect CI increases with fluid loading was greatest when GEF was ≤20% (in 53% of patients).
Conclusions: An increase in SvO2 ≥2%, irrespective of a relatively high baseline value, can thus be used as a monitor of fluid responsiveness in clinically hypovolemic patients after cardiac or major vascular surgery, particularly in those with systolic cardiac dysfunction. Fluid responsiveness concurs with increased tissue O2 delivery.
Figures
References
-
- Gattinoni L, Brazzi L, Pelosi P, Latini R, Tognoni G, Pesenti A, Fumagalli R. for the SvO2 collaborative group. A trial of goal-oriented hemodynamic therapy in critically ill patients. N Engl J Med. 1995;16:1025–1032. - PubMed
-
- Verheij J, van Lingen A, Beishuizen A, Christiaans HM, de Jong JR, Girbes AR, Wisselink W, Rauwerda JA, Huybregts MA, Groeneveld AB. Cardiac response is greater for colloid than saline fluid loading after cardiac or vascular surgery. Intensive Care Med. 2006;32:1030–1038. doi: 10.1007/s00134-006-0195-5. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
