

Efficacy of combination of Ezetimibe 10 mg and rosuvastatin 2.5 mg versus rosuvastatin 5 mg monotherapy for hypercholesterolemia in patients with type 2 diabetes
- PMID: 24053480
- PMCID: PMC3849617
- DOI: 10.1186/1476-511X-12-137
Efficacy of combination of Ezetimibe 10 mg and rosuvastatin 2.5 mg versus rosuvastatin 5 mg monotherapy for hypercholesterolemia in patients with type 2 diabetes
Abstract
Background: Statins are used to treat hypercholesterolemia in patients with type 2 diabetes mellitus, but many of these patients fail to achieve the target LDL-C level. Recent reports have suggested that a synergistic effect can be obtained by concomitant administration of the cholesterol absorption inhibitor ezetimibe and a statin. However, in patients with type 2 diabetes who are already being treated with satins, it remains unclear whether it is more effective to add ezetimibe or to increase the statin dose. Therefore, this study was performed to examine the effects of these two regimens on LDL-C and lipoproteins.
Methods: The subjects were type 2 diabetic patients under treatment with rosuvastatin (2.5 mg daily), who had LDL-C levels ≥80 mg/dL. They were randomly allocated to a group that received add-on therapy with ezetimibe at 10 mg/day (combination group, n = 40) or an increase of the rosuvastatin dose to 5 mg/day (dose escalation group, n = 39). These two groups were compared at baseline and after 12 weeks of treatment.
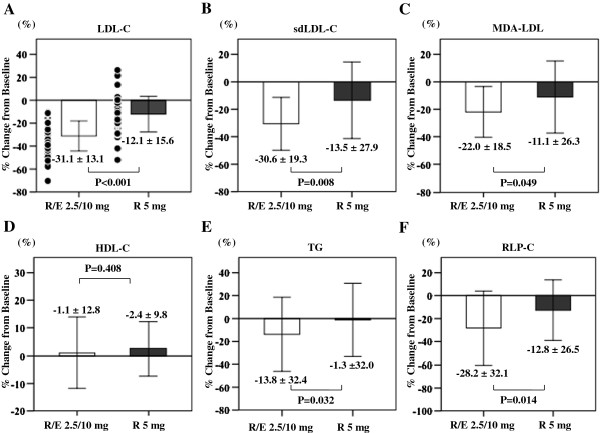
Results: The percent change of LDL-C was -31% in the combination group and -12% in the dose escalation group. Both groups showed a significant decrease, but the decrease was greater in the combination group. In both groups, there was a significant decrease in the levels of small dense LDL-C, oxidized LDL and remnant-like lipoprotein cholesterol. For all of these parameters, the percent changes were greater in the combination group. Only the combination group showed a significant decrease of triglycerides. Multivariate analysis was performed to identify factors associated with reaching an LDL-C level <80 mg/dL. As a result, add-on therapy with ezetimibe was extracted as a factor related to improvement of LDL-C.
Conclusions: Compared with increasing the dose of rosuvastatin, the combination of rosuvastatin and ezetimibe not only achieves quantitative but also qualitative improvement of serum lipid levels in type 2 diabetic patients, suggesting that this combination could suppress the progression of atherosclerosis.
Trial registration: UMIN000011005.
Figures
Similar articles
-
Changes in LDL-C levels and goal attainment associated with addition of ezetimibe to simvastatin, atorvastatin, or rosuvastatin compared with titrating statin monotherapy.Vasc Health Risk Manag. 2013;9:719-27. doi: 10.2147/VHRM.S49840. Epub 2013 Nov 15. Vasc Health Risk Manag. 2013. PMID: 24265554 Free PMC article.
-
Pharmacodynamic interaction between ezetimibe and rosuvastatin.Curr Med Res Opin. 2004 Aug;20(8):1185-95. doi: 10.1185/030079904125004213. Curr Med Res Opin. 2004. PMID: 15324521 Clinical Trial.
-
Comparison of anti-inflammatory effects and high-density lipoprotein cholesterol levels between therapy with quadruple-dose rosuvastatin and rosuvastatin combined with ezetimibe.Lipids Health Dis. 2013 Feb 4;12:9. doi: 10.1186/1476-511X-12-9. Lipids Health Dis. 2013. PMID: 23374898 Free PMC article. Clinical Trial.
-
Newer pharmaceutical agents to treat lipid disorders.Curr Cardiol Rep. 2003 Nov;5(6):463-9. doi: 10.1007/s11886-003-0108-y. Curr Cardiol Rep. 2003. PMID: 14558988 Review.
-
Lipid-altering efficacy of ezetimibe plus statin and statin monotherapy and identification of factors associated with treatment response: a pooled analysis of over 21,000 subjects from 27 clinical trials.Atherosclerosis. 2012 Aug;223(2):251-61. doi: 10.1016/j.atherosclerosis.2012.02.016. Epub 2012 Feb 16. Atherosclerosis. 2012. PMID: 22410123 Review.
Cited by
-
Combination Therapy of Ezetimibe and Rosuvastatin for Dyslipidemia: Current Insights.Drug Des Devel Ther. 2022 Jul 7;16:2177-2186. doi: 10.2147/DDDT.S332352. eCollection 2022. Drug Des Devel Ther. 2022. PMID: 35832642 Free PMC article. Review.
-
The Effects of Statin Dose, Lipophilicity, and Combination of Statins plus Ezetimibe on Circulating Oxidized Low-Density Lipoprotein Levels: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Mediators Inflamm. 2021 Sep 4;2021:9661752. doi: 10.1155/2021/9661752. eCollection 2021. Mediators Inflamm. 2021. PMID: 34526854 Free PMC article.
-
Efficacy and Tolerability of a Fixed-Dose Combination of Rosuvastatin and Ezetimibe Compared with a Fixed-Dose Combination of Simvastatin and Ezetimibe in Brazilian Patients with Primary Hypercholesterolemia or Mixed Dyslipidemia: A Multicenter, Randomized Trial.Curr Ther Res Clin Exp. 2020 Jul 28;93:100595. doi: 10.1016/j.curtheres.2020.100595. eCollection 2020. Curr Ther Res Clin Exp. 2020. PMID: 32904162 Free PMC article.
-
Atherogenic Lipoproteins for the Statin Residual Cardiovascular Disease Risk.Int J Mol Sci. 2022 Nov 4;23(21):13499. doi: 10.3390/ijms232113499. Int J Mol Sci. 2022. PMID: 36362288 Free PMC article. Review.
-
Effect of fixed-dose combinations of ezetimibe plus rosuvastatin in patients with primary hypercholesterolemia: MRS-ROZE (Multicenter Randomized Study of ROsuvastatin and eZEtimibe).Cardiovasc Ther. 2016 Oct;34(5):371-82. doi: 10.1111/1755-5922.12213. Cardiovasc Ther. 2016. PMID: 27506635 Free PMC article. Clinical Trial.
References
-
- Sone H, Tanaka S, Tanaka S. et al.Serum level of triglycerides is a potent risk factor comparable to LDL cholesterol for coronary heart disease in Japanese patients with type 2 diabetes: subanalysis of the Japan diabetes complications study (JDCS) J Clin Endocrinol Metab. 2011;96:3448–3456. - PubMed
-
- Teramoto T, Kashiwagi A, Mabuchi H. Status of lipid-lowering therapy prescribed based on recommendations in the 2002 report of the Japan atherosclerosis society guideline for diagnosis and treatment of hyperlipidemia in Japanese adults: a study of the Japan lipid assessment program (J-LAP) Curr Ther Res Clin Exp. 2005;66:80–95. - PMC - PubMed
-
- Altmann SW, Davis HR Jr, Zhu LJ. et al.Niemann-Pick C1 Like 1 protein is critical for intestinal cholesterol absorption. Science. 2004;303:1201–1204. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
