

Cytoreductive nephrectomy in patients with metastatic non-clear-cell renal cell carcinoma (RCC)
- PMID: 24053727
- PMCID: PMC4117702
- DOI: 10.1111/bju.12442
Cytoreductive nephrectomy in patients with metastatic non-clear-cell renal cell carcinoma (RCC)
Abstract
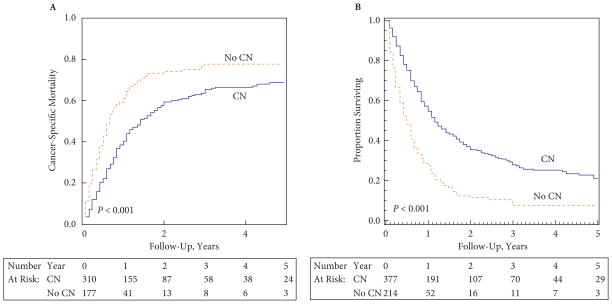
Objective: To determine whether patients with metastatic non-clear-cell renal cell carcinoma (RCC) benefit from cytoreductive nephrectomy (CN).
Patients and methods: We used the Surveillance, Epidemiology, and End Results (SEER) programme to identify a population-based sample of 4914 patients diagnosed with metastatic RCC between 2000 and 2009. Of the 4914 patients, 591 had non-clear-cell histology. The median follow-up was 20 months. The primary outcome measure was RCC-specific mortality.
Results: Approximately 64% of patients underwent CN. Patients with non-clear-cell histology who underwent CN had lower RCC-specific and all-cause mortality than those who did not (P < 0.001 in both cases). After adjustment for age, gender, race, marital status, year of diagnosis, geographical location and histology, the associations between CN and lower RCC-specific mortality (hazard ratio [HR] 0.62, 95% confidence interval [CI] 0.48-0.80, P < 0.001) and between CN and all-cause mortality (HR 0.45, 95% CI 0.37-0.55, P < 0.001) remained highly significant. Among patients diagnosed between 2006 and 2009 (targeted therapy era), the results remained unchanged (HR 0.50, 95% CI 0.34-0.72, P < 0.001 and HR 0.43, 95% CI 0.31-0.59, P < 0.001, respectively). An interaction model found lower all-cause mortality for all histologies after CN.
Conclusions: Patients from the SEER programme with metastatic non-clear-cell RCC, including those treated in the targeted therapy era, appear to derive a survival benefit from CN, an association which remained significant regardless of histological subtype. This observation suggests that CN should remain standard in patients with advanced RCC who are deemed to be surgical candidates.
Keywords: clear cell; cytoreductive nephrectomy; mortality; non-clear-cell; renal cell carcinoma; survival.
© 2013 The Authors. BJU International © 2013 BJU International.
Conflict of interest statement
There was no external financial support for this study. T.C. is a Consultant and/or on an Advisory Board for Pfizer Inc., Bayer AG, GlaxoSmithKline and Novartis. P.N. declares research funding from Varian Consulting, Ferring Inc., Astellas Pharma and Medivation. No other conflicts of interest declared.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Rini BI, Campbell SC, Escudier B. Renal cell carcinoma. Lancet. 2009;373:1119–32. - PubMed
-
- Escudier B, Eisen T, Stadler WM, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;356:125–34. - PubMed
-
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115–24. - PubMed
-
- Flanigan RC, Salmon SE, Blumenstein BA, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer. N Engl J Med. 2001;345:1655–9. - PubMed
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
