

Comparison of strategies to reduce meticillin-resistant Staphylococcus aureus rates in surgical patients: a controlled multicentre intervention trial
- PMID: 24056477
- PMCID: PMC3780302
- DOI: 10.1136/bmjopen-2013-003126
Comparison of strategies to reduce meticillin-resistant Staphylococcus aureus rates in surgical patients: a controlled multicentre intervention trial
Abstract
Objective: To compare the effect of two strategies (enhanced hand hygiene vs meticillin-resistant Staphylococcus aureus (MRSA) screening and decolonisation) alone and in combination on MRSA rates in surgical wards.
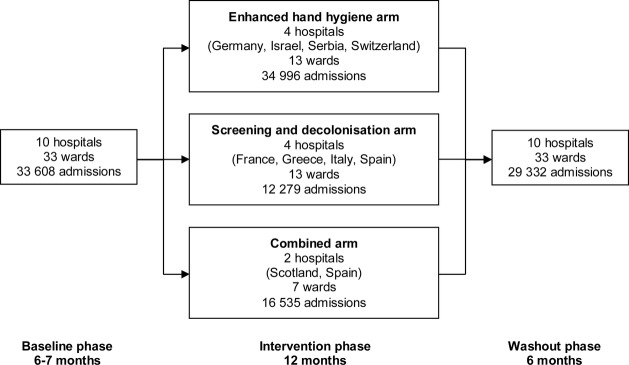
Design: Prospective, controlled, interventional cohort study, with 6-month baseline, 12-month intervention and 6-month washout phases.
Setting: 33 surgical wards of 10 hospitals in nine countries in Europe and Israel.
Participants: All patients admitted to the enrolled wards for more than 24 h.
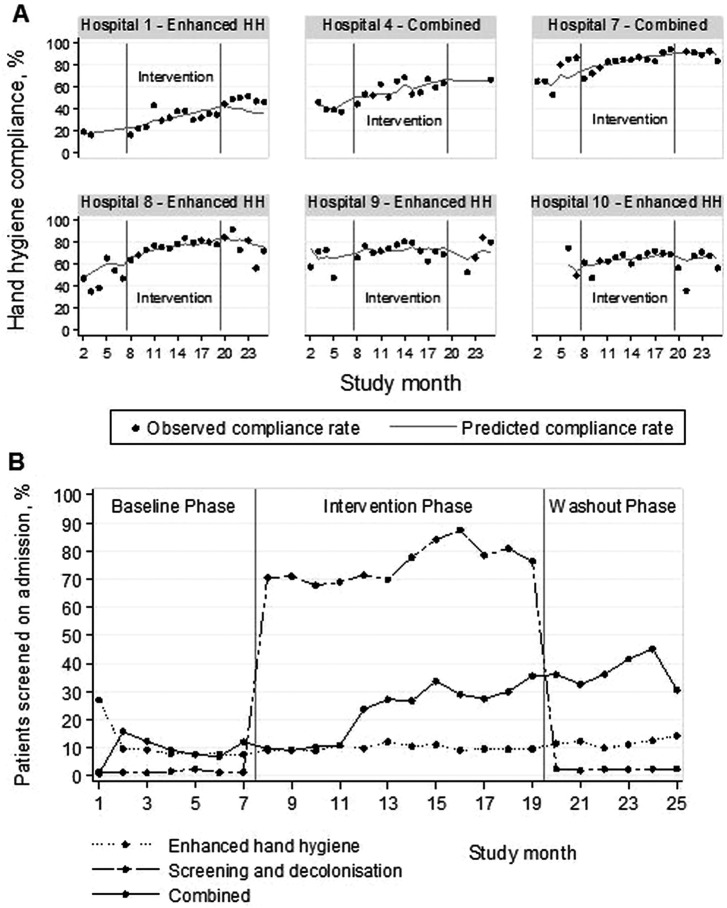
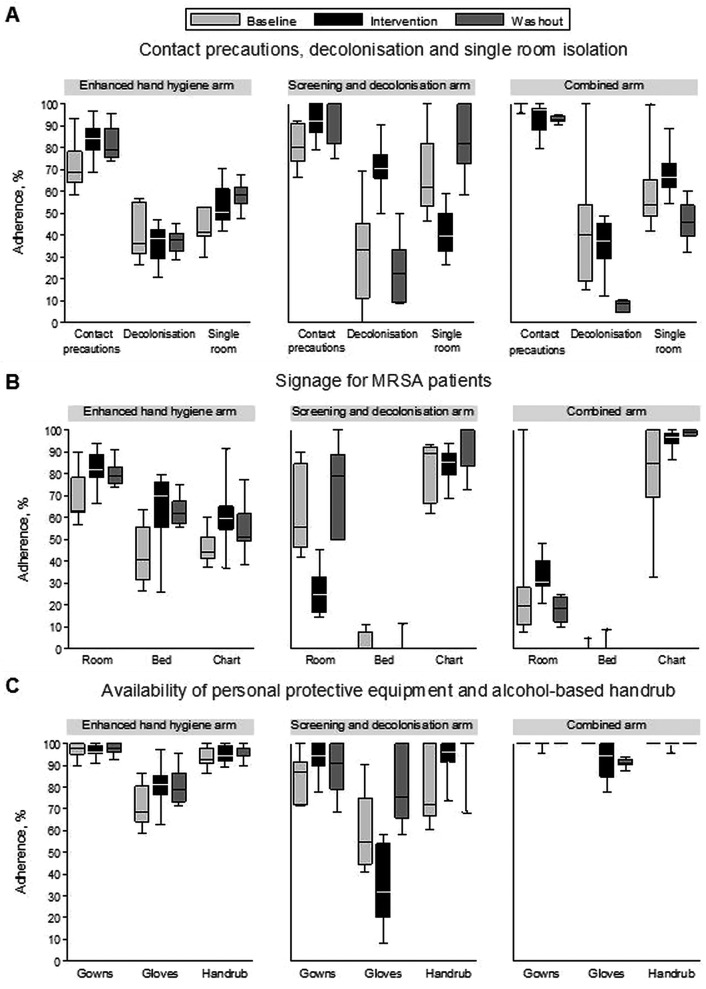
Interventions: The two strategies compared were (1) enhanced hand hygiene promotion and (2) universal MRSA screening with contact precautions and decolonisation (intranasal mupirocin and chlorhexidine bathing) of MRSA carriers. Four hospitals were assigned to each intervention and two hospitals combined both strategies, using targeted MRSA screening.
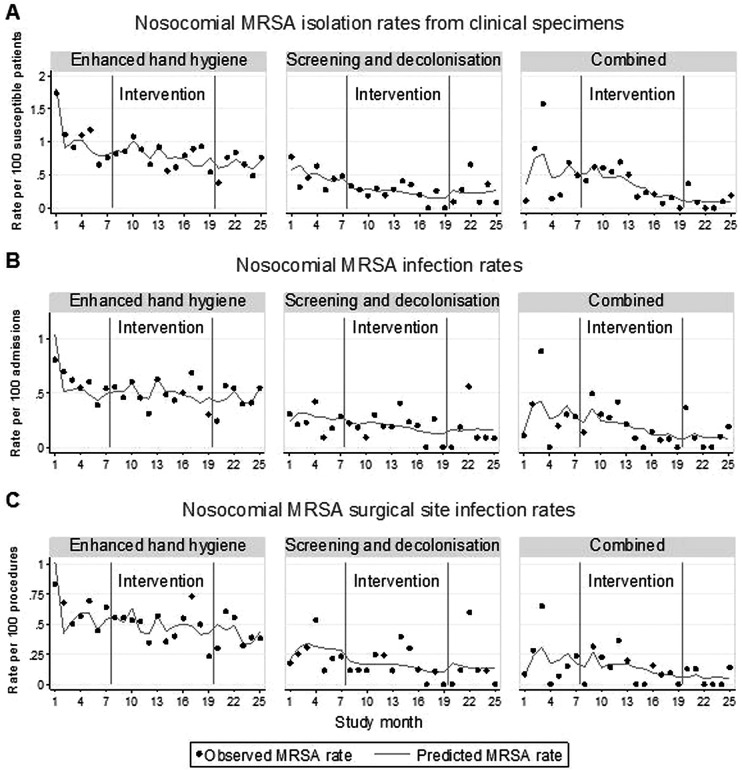
Outcome measures: Monthly rates of MRSA clinical cultures per 100 susceptible patients (primary outcome) and MRSA infections per 100 admissions (secondary outcome). Planned subgroup analysis for clean surgery wards was performed.
Results: After adjusting for clustering and potential confounders, neither strategy when used alone was associated with significant changes in MRSA rates. Combining both strategies was associated with a reduction in the rate of MRSA clinical cultures of 12% per month (adjusted incidence rate ratios (aIRR) 0.88, 95% CI 0.79 to 0.98). In clean surgery wards, strategy 2 (MRSA screening, contact precautions and decolonisation) was associated with decreasing rates of MRSA clinical cultures (15% monthly decrease, aIRR 0.85, 95% CI 0.74 to 0.97) and MRSA infections (17% monthly decrease, aIRR 0.83, 95% CI 0.69 to 0.99).
Conclusions: In surgical wards with relatively low MRSA prevalence, a combination of enhanced standard and MRSA-specific infection control approaches was required to reduce MRSA rates. Implementation of single interventions was not effective, except in clean surgery wards where MRSA screening coupled with contact precautions and decolonisation was associated with significant reductions in MRSA clinical culture and infection rates.
Trial registration: clinicaltrials.gov identifier: NCT00685867.
Keywords: Infection Control < Infectious Diseases; Surgery.
Figures
References
-
- WHO Report on the burden of endemic health care-associated infection worldwide. http://whqlibdoc.who.int/publications/2011/9789241501507_eng.pdf (accessed 24 Apr 2013).
-
- Cosgrove SE, Qi Y, Kaye KS, et al. The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges. Infect Control Hosp Epidemiol 2005;26:166–74 - PubMed
-
- Weber SG, Huang SS, Oriola S, et al. Legislative mandates for use of active surveillance cultures to screen for methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci: position statement from the joint SHEA and APIC task force. Am J Infect Control 2007;35:73–85 - PubMed
-
- UK Department of Health MRSA Screening—Operational Guidance 2. http://www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/De... (accessed 24 Apr 2013).
-
- Robicsek A, Beaumont JL, Paule SM, et al. Universal surveillance for methicillin-resistant Staphylococcus aureus in 3 affiliated hospitals. Ann Intern Med 2008;148:409–18 - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical