

Surgical resection of epidural disease improves local control following postoperative spine stereotactic body radiotherapy
- PMID: 24057886
- PMCID: PMC3779044
- DOI: 10.1093/neuonc/not101
Surgical resection of epidural disease improves local control following postoperative spine stereotactic body radiotherapy
Abstract
Background: Spine stereotactic body radiotherapy (SBRT) is increasingly being applied to the postoperative spine metastases patient. Our aim was to identify clinical and dosimetric predictors of local control (LC) and survival.
Methods: Eighty patients treated between October 2008 and February 2012 with postoperative SBRT were identified from our prospective database and retrospectively reviewed.
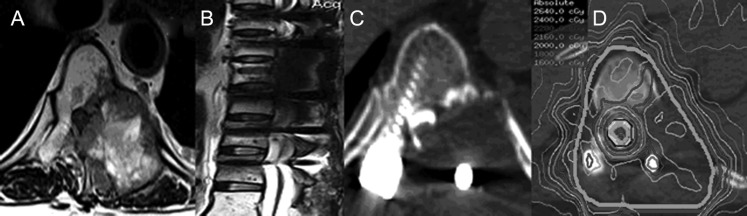
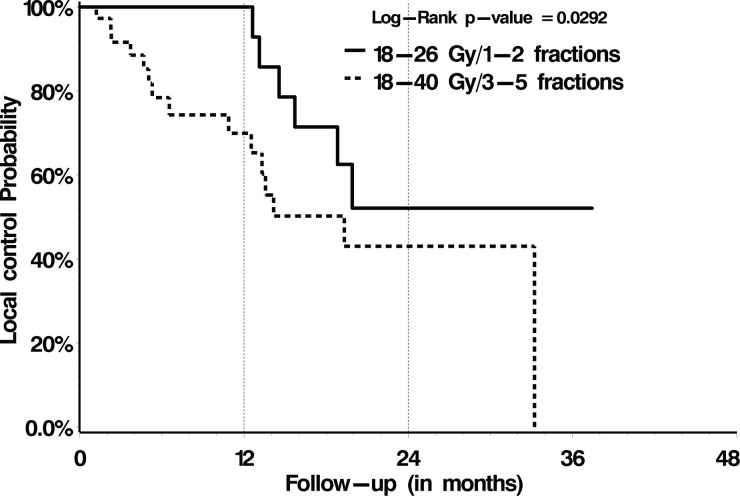
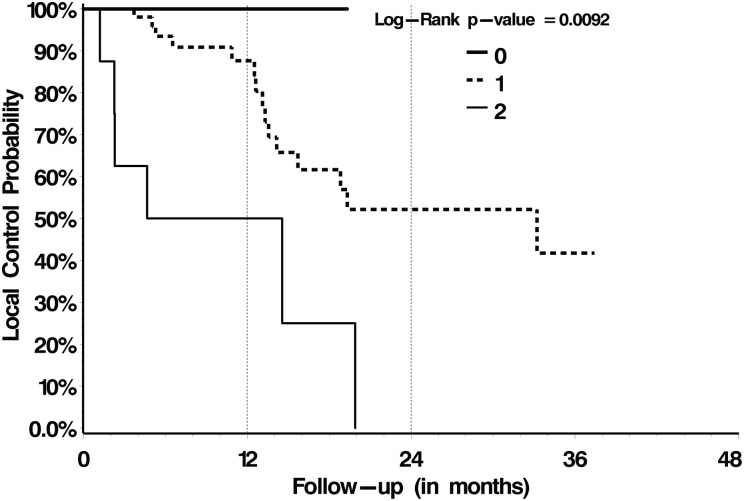
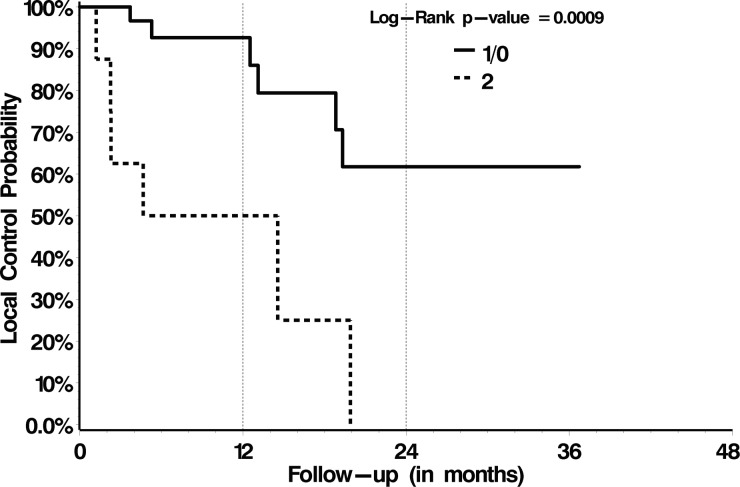
Results: The median follow-up was 8.3 months. Thirty-five patients (44%) were treated with 18-26 Gy in 1 or 2 fractions, and 45 patients (56%) with 18-40 Gy in 3-5 fractions. Twenty-one local failures (26%) were observed, and the 1-year LC and overall survival (OS) rates were 84% and 64%, respectively. The most common site of failure was within the epidural space (15/21, 71%). Multivariate proportional hazards analysis identified systemic therapy post-SBRT as the only significant predictor of OS (P = .02) and treatment with 18-26 Gy/1 or 2 fractions (P = .02) and a postoperative epidural disease grade of 0 or 1 (0, no epidural disease; 1, epidural disease that compresses dura only, P = .003) as significant predictors of LC. Subset analysis for only those patients (n = 48/80) with high-grade preoperative epidural disease (cord deformed) indicated significantly greater LC rates when surgically downgraded to 0/1 vs 2 (P = .0009).
Conclusions: Postoperative SBRT with high total doses ranging from 18 to 26 Gy delivered in 1-2 fractions predicted superior LC, as did postoperative epidural grade.
Keywords: postoperative radiation; spinal cord compression; spine metastases; spine radiosurgery; spine stereotactic body radiotherapy.
Figures
References
-
- Patchell RA, Tibbs PA, Regine WF, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 2005;366:643–648. - PubMed
-
- Klekamp J, Samii H. Surgical results for spinal metastases. Acta Neurochir (Wien) 1998;140:957–967. - PubMed
-
- Missenard G, Lapresle P, Cote D. Local control after surgical treatment of spinal metastatic disease. Eur Spine J. 1996;5:45–50. - PubMed
-
- Rades D, Huttenlocher S, Bajrovic A, et al. Surgery followed by radiotherapy versus radiotherapy alone for metastatic spinal cord compression from unfavorable tumors. Int J Radiat Oncol Biol Phys. 2011;81:e861–e868. - PubMed
-
- Sahgal A, Bilsky M, Chang EL, et al. Stereotactic body radiotherapy for spinal metastases: current status, with a focus on its application in the postoperative patient. J Neurosurg Spine. 2011;14:151–166. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
