

Challenges and implications of routine depression screening for depression in chronic disease and multimorbidity: a cross sectional study
- PMID: 24058602
- PMCID: PMC3772931
- DOI: 10.1371/journal.pone.0074610
Challenges and implications of routine depression screening for depression in chronic disease and multimorbidity: a cross sectional study
Abstract
Background: Depression screening in chronic disease is advocated but its impact on routine practice is uncertain. We examine the effects of a programme of incentivised depression screening in chronic disease within a UK primary care setting.
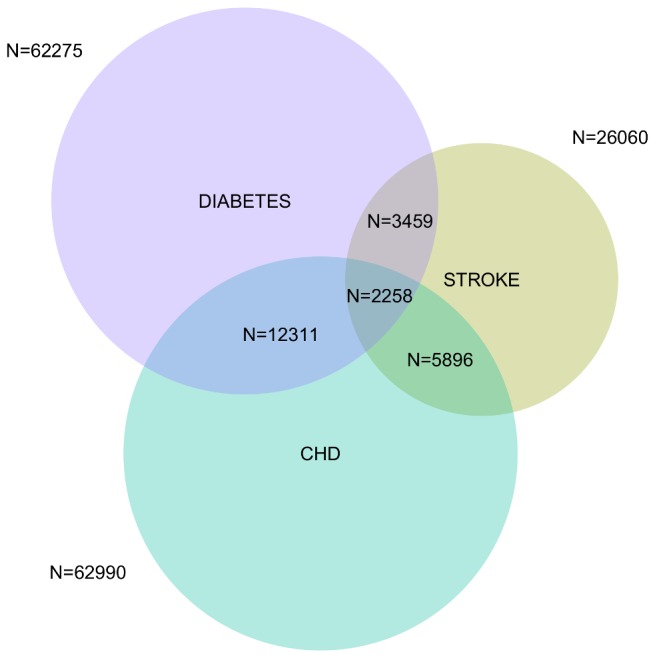
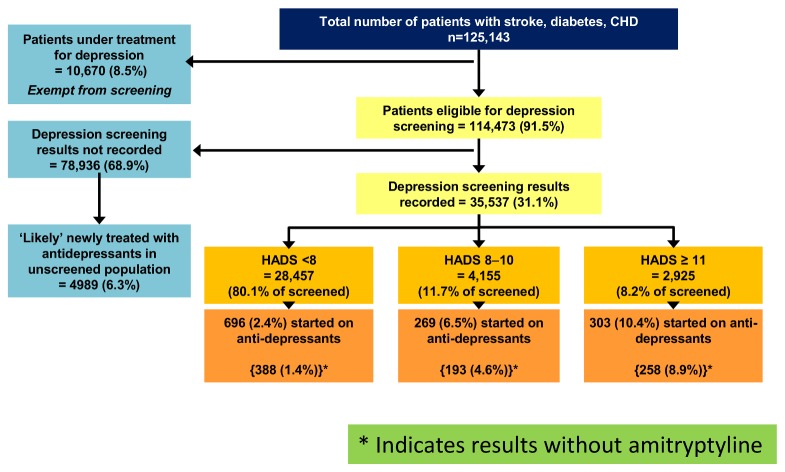
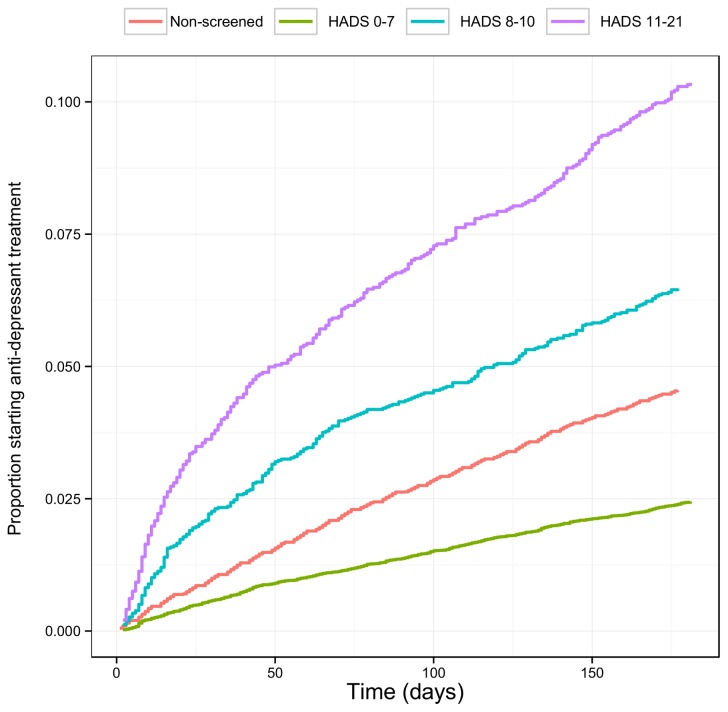
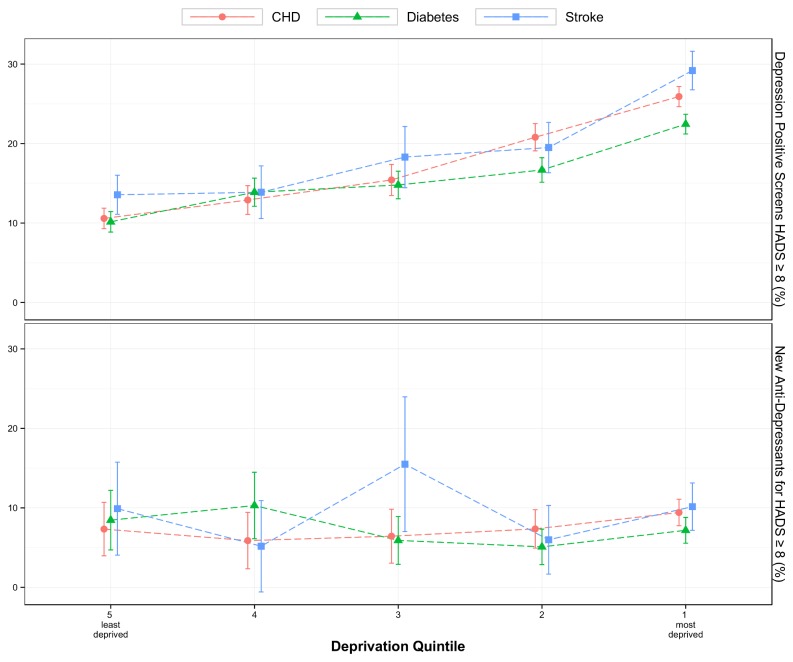
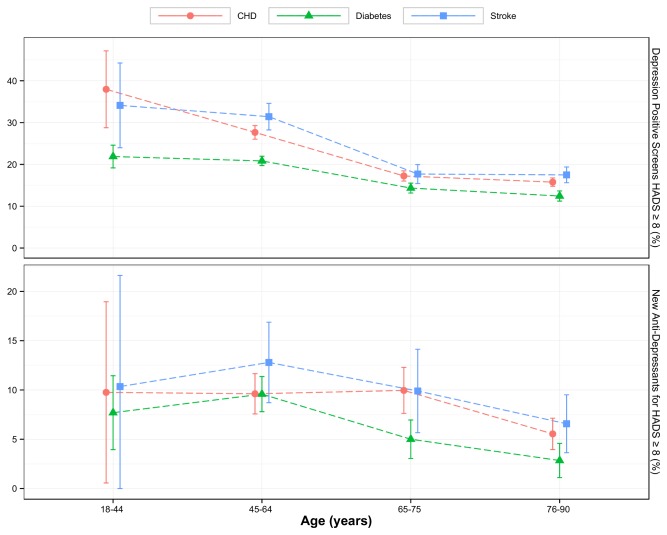
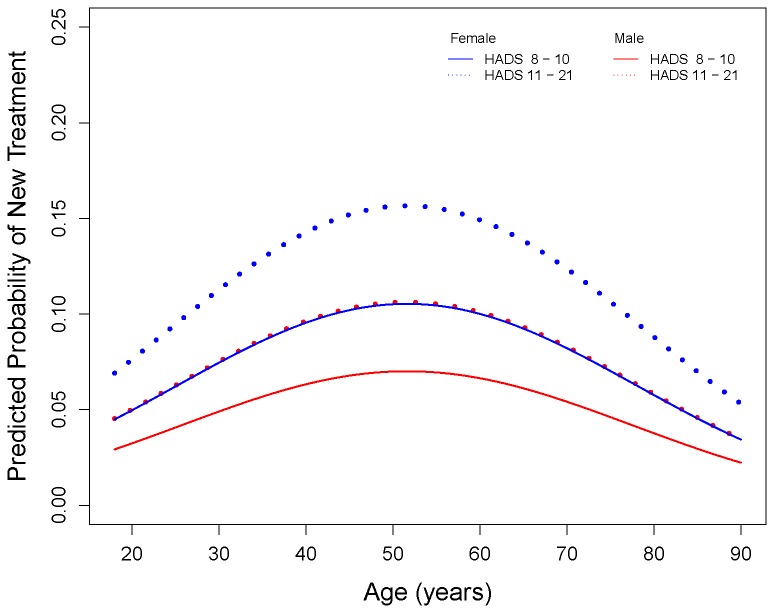
Methods and findings: Cross sectional analysis of anonymised, routinely collected data (2008-9) from family practices in Scotland serving a population of circa 1.8 million. Primary care registered patients with at least one of three chronic diseases, coronary heart disease, diabetes and stroke, underwent incentivised depression screening using the Hospital Anxiety and Depression Score (HADS). 125143 patients were identified with at least one chronic disease. 10670 (8.5%) were under treatment for depression and exempt from screening. Of remaining, HADS were recorded for 35537 (31.1%) patients. 7080 (19.9% of screened) had raised HADS (≥8); majority had indications of mild depression with HADS between 8 and 10. Over 6 months, 572 (8%) of those with raised HADS (≥8) were initiated on antidepressants, while 696 (2.4%) patients with normal HADS (<8) were also initiated on antidepressants (relative risk of antidepressant initiation with raised HADS 3.3 (CI 2.97-3.67), p value <0.0001). Of those with multimorbidity who were screened, 24.3% had raised HADS (≥8). A raised HADS was more likely in females, socioeconomically deprived, multimorbid or younger (18-44) individuals. Females and 45-64 years old were more likely to receive antidepressants.
Limitations: retrospective study of routinely collected data.
Conclusions: Despite incentivisation, only a minority of patients underwent depression screening, suggesting that systematic depression screening in chronic disease can be difficult to achieve in routine practice. Targeting those at greatest risk such as the multimorbid or using simpler screening methods may be more effective. Raised HADS was associated with higher number of new antidepressant prescriptions which has significant resource implications. The clinical benefits of such screening remain uncertain and merits investigation.
Conflict of interest statement
Figures
References
-
- Egede LE (2007) Major depression in individuals with chronic medical disorders: prevalence, correlates and association with health resource utilization, lost productivity and functional disability. Gen Hosp Psychiatry 29: 409-416. doi:10.1016/j.genhosppsych.2007.06.002. PubMed: 17888807. - DOI - PubMed
-
- Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B (2007) Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet 370: 851-858. doi:10.1016/S0140-6736(07)61415-9. PubMed: 17826170. - DOI - PubMed
-
- Mitchell AJ, Ferguson DW, Gill J, Paul J, Symonds P (2013) Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: a systematic review and meta-analysis. Lancet Oncol 14: 721-732. S1470- doi:10.1016/S1470-2045(13)70244-4. PubMed: 23759376. 2045(13)70244-4 . PII . doi:10.1016/S1470-2045(13)70244-4 - DOI - DOI - PubMed
-
- Ali S, Stone MA, Peters JL, Davies MJ, Khunti K (2006) The prevalence of co-morbid depression in adults with Type 2 diabetes: a systematic review and meta-analysis. Diabet Med 23: 1165-1173. doi:10.1111/j.1464-5491.2006.01943.x. PubMed: 17054590. - DOI - PubMed
-
- Hadidi N, Treat-Jacobson DJ, Lindquist R (2009) Poststroke depression and functional outcome: a critical review of literature. Heart Lung 38: 151-162. doi:10.1016/j.hrtlng.2008.05.002. PubMed: 19254633. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
