

Heterogeneity of estrogen receptor expression in circulating tumor cells from metastatic breast cancer patients
- PMID: 24058649
- PMCID: PMC3776726
- DOI: 10.1371/journal.pone.0075038
Heterogeneity of estrogen receptor expression in circulating tumor cells from metastatic breast cancer patients
Abstract
Background: Endocrine treatment is the most preferable systemic treatment in metastatic breast cancer patients that have had an estrogen receptor (ER) positive primary tumor or metastatic lesions, however, approximately 20% of these patients do not benefit from the therapy and demonstrate further metastatic progress. One reason for failure of endocrine therapy might be the heterogeneity of ER expression in tumor cells spreading from the primary tumor to distant sites which is reflected in detectable circulating tumor cells (CTCs).
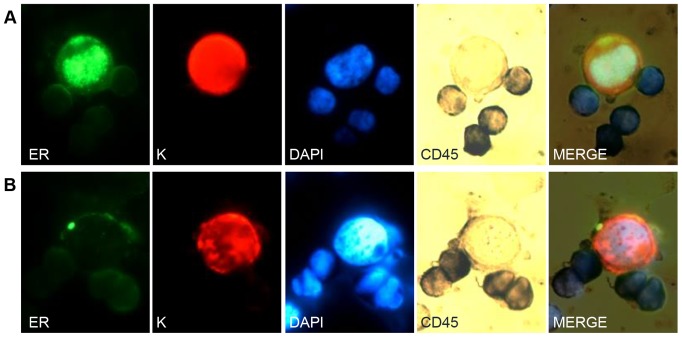
Methods: A sensitive and specific staining protocol for ER, keratin 8/18/19, CD45 was established. Peripheral blood from 35 metastatic breast cancer patients with ER-positive primary tumors was tested for the presence of CTCs. Keratin 8/18/19 and DAPI positive but CD45 negative cells were classified as CTCs and evaluated for ER staining. Subsequently, eight individual CTCs from four index patients (2 CTCs per patient) were isolated and underwent whole genome amplification and ESR1 gene mutation analysis.
Results: CTCs were detected in blood of 16 from 35 analyzed patients (46%), with a median of 3 CTCs/7.5 ml. In total, ER-negative CTCs were detected in 11/16 (69%) of the CTC positive cases, including blood samples with only ER-negative CTCs (19%) and samples with both ER-positive and ER-negative CTCs (50%). No correlation was found between the intensity and/or percentage of ER staining in the primary tumor with the number and ER status of CTCs of the same patient. ESR1 gene mutations were not found.
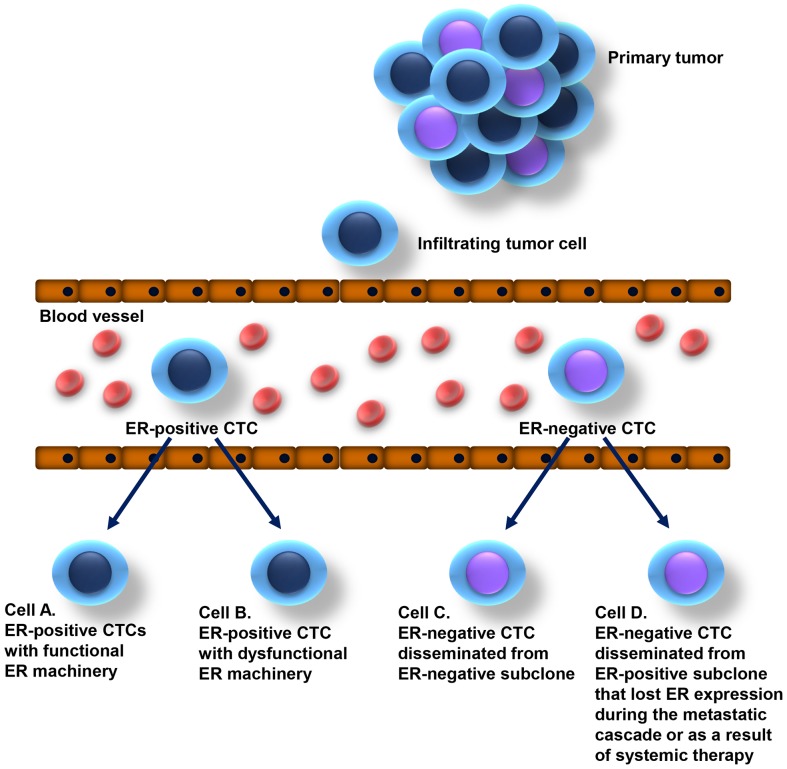
Conclusion: CTCs frequently lack ER expression in metastatic breast cancer patients with ER-positive primary tumors and show a considerable intra-patient heterogeneity, which may reflect a mechanism to escape endocrine therapy. Provided single cell analysis did not support a role of ESR1 mutations in this process.
Conflict of interest statement
Figures
References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, et al. (2010) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127: 2893–2917 doi:10.1002/ijc.25516 - DOI - PubMed
-
- Eroles P, Bosch A, Perez-Fidalgo JA, Lluch A (2012) Molecular biology in breast cancer: Intrinsic subtypes and signaling pathways. Cancer Treat Rev 38: 698–707. S0305-7372(11)00244-1 [pii] doi:10.1016/j.ctrv.2011.11.005 - DOI - PubMed
-
- Nielsen TO, Hsu FD, Jensen K, Cheang M, Karaca G, et al. (2004) Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin Cancer Res 10: 5367–5374. 10/16/5367 [pii]. doi:10.1158/1078-0432.CCR-04-0220 - DOI - PubMed
-
- Park S, Koo JS, Kim MS, Park HS, Lee JS, et al. (2012) Characteristics and outcomes according to molecular subtypes of breast cancer as classified by a panel of four biomarkers using immunohistochemistry. Breast 21: 50–57. S0960-9776(11)00158-5 [pii]; doi:10.1016/j.breast.2011.07.008 - DOI - PubMed
-
- Joosse SA (2012) BRCA1 and BRCA2: a common pathway of genome protection but different breast cancer subtypes. Nat Rev Cancer 12: 372 nrc3181-c2 [pii]; doi:10.1038/nrc3181-c2 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
