

Food allergy and increased asthma morbidity in a School-based Inner-City Asthma Study
- PMID: 24058900
- PMCID: PMC3777668
- DOI: 10.1016/j.jaip.2013.06.007
Food allergy and increased asthma morbidity in a School-based Inner-City Asthma Study
Abstract
Background: Children with asthma have increased prevalence of food allergies. The relationship between food allergy and asthma morbidity is unclear.
Objective: We aimed to investigate the presence of food allergy as an independent risk factor for increased asthma morbidity by using the School Inner-City Asthma Study, a prospective study that evaluates risk factors and asthma morbidity among urban children.
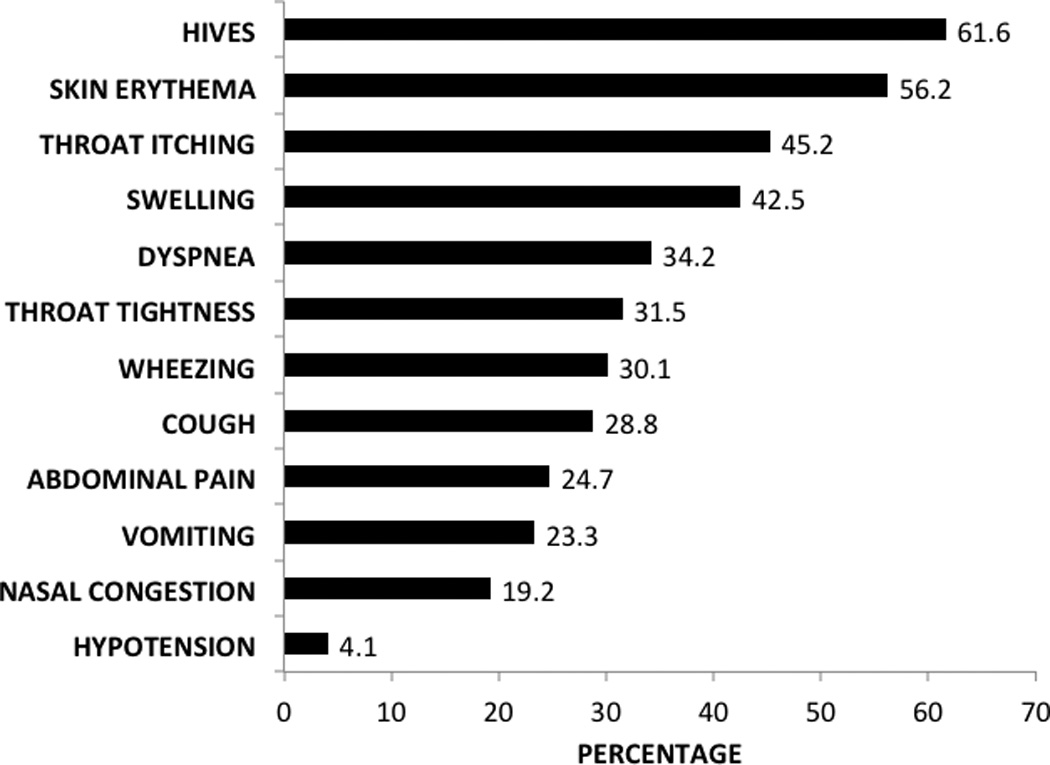
Methods: We prospectively surveyed, from inner-city schools, 300 children with physician-diagnosed asthma, followed by clinical evaluation. Food allergies were reported, which included symptoms experienced within 1 hour of food ingestion. Asthma morbidity, pulmonary function, and resource utilization were compared between children with food allergies and those without.
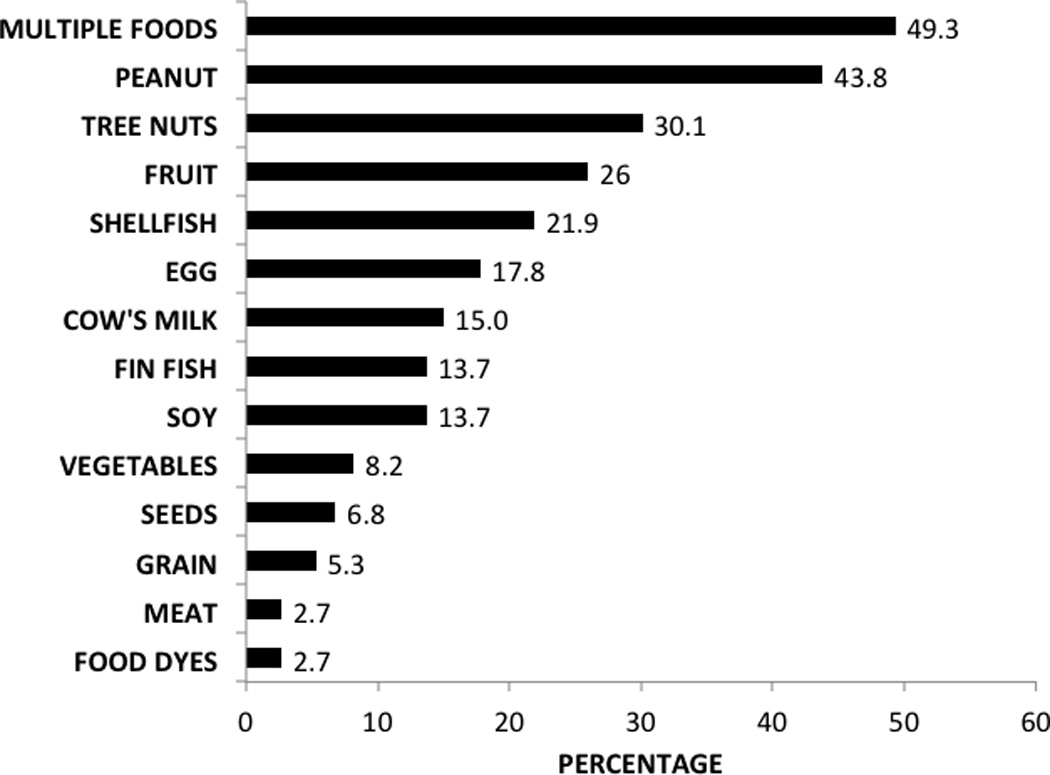
Results: Seventy-three of 300 children with asthma (24%) surveyed had physician-diagnosed food allergy, and 36 (12%) had multiple food allergies. Those with any food allergy independently had increased risk of hospitalization (OR [odds ratio] 2.35 [95% CI, 1.30-4.24]; P = .005) and use of controller medication (OR 1.99 [95% CI, 1.06-3.74]; P = .03). Those with multiple food allergies also had an independently higher risk of hospitalization in the past year (OR 4.10 [95% CI, 1.47-11.45]; P = .007), asthma-related hospitalization (OR 3.52 [95% CI, 1.12-11.03]; P = .03), controller medication use (OR 2.38 [95% CI, 1.00-5.66]; P = .05), and more provider visits (median, 4.5 vs 3.0; P = .008). Furthermore, lung function was significantly lower (percent predicted FEV1 and FEV1/FVC ratios) in both food allergy category groups.
Conclusions: Food allergy is highly prevalent in inner-city school-aged children with asthma. Children with food allergies have increased asthma morbidity and health resource utilization with decreased lung function, and this association is stronger in those with multiple food allergies.
Copyright © 2013 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Pleis JR, Ward BW, Lucas JW. Summary health statistics for U.S. adults: National Health Interview Survey, 2009. Vital Health Stat. 2010;10(249):1–207. - PubMed
-
- Bloom B, Cohen RA, Freeman G. Summary health statistics for U.S. children: National Health Interview Survey, 2009. Vital Health Stat. 2010;10(247):1–82. - PubMed
-
- Akinbami LJ, Moorman JE, Bailey C, et al. Trends in asthma prevalence, health care use, and mortality in the United States, 2001–2010. NCHS Data Brief. 2012;(94):1–8. - PubMed
-
- Akinbami LJ, Moorman JE, Liu X. Asthma prevalence, health care use, and mortality: United States, 2005–2009. Natl Health Stat Report. 2011;(32):1–14. - PubMed
-
- Branum AM, Lukacs SL. Food allergy among children in the United States. Pediatrics. 2009;124(6):1549–1555. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous