

Prostate specific antigen velocity risk count predicts biopsy reclassification for men with very low risk prostate cancer
- PMID: 24060641
- PMCID: PMC4711358
- DOI: 10.1016/j.juro.2013.09.029
Prostate specific antigen velocity risk count predicts biopsy reclassification for men with very low risk prostate cancer
Abstract
Purpose: Prostate specific antigen velocity is an unreliable predictor of adverse pathology findings in patients on active surveillance for low risk prostate cancer. However, to our knowledge a new concept called prostate specific antigen velocity risk count, recently validated in a screening cohort, has not been investigated in an active surveillance cohort.
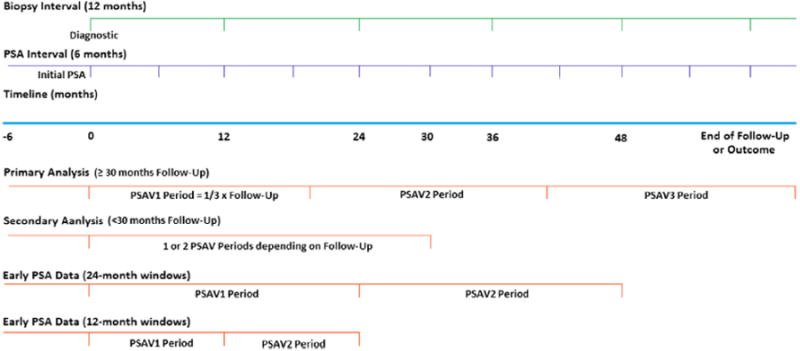
Materials and methods: We evaluated a cohort of men from 1995 to 2012 with prostate cancer on active surveillance. They had stage T1c disease, prostate specific antigen density less than 0.15 ng/ml, Gleason score 6 or less, 2 or fewer biopsy cores and 50% or less involvement of any core with cancer. The men were observed by semiannual prostate specific antigen measurements, digital rectal examinations and an annual surveillance biopsy. Treatment was recommended for biopsy reclassification. Patients with 30 months or greater of followup and 3 serial prostate specific antigen velocity measurements were used in primary analysis by logistic regression, Cox proportional hazards, Kaplan-Meier analysis and performance parameters, including the AUC of the ROC curve.
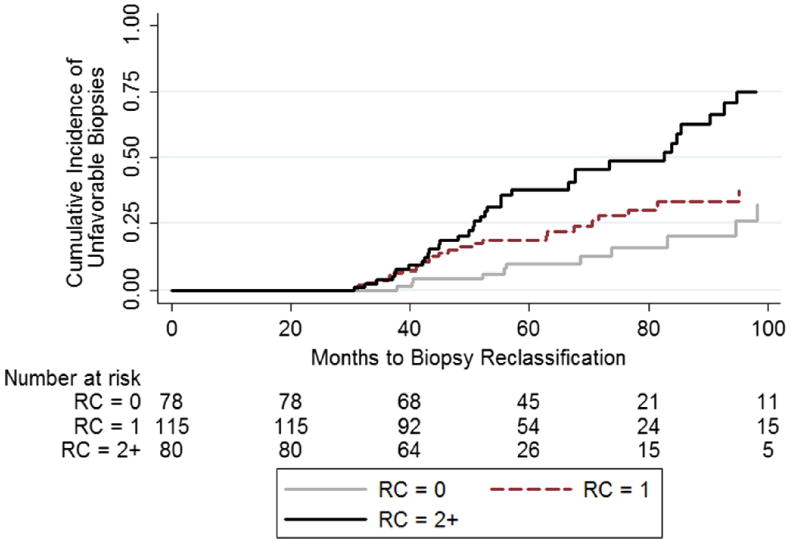
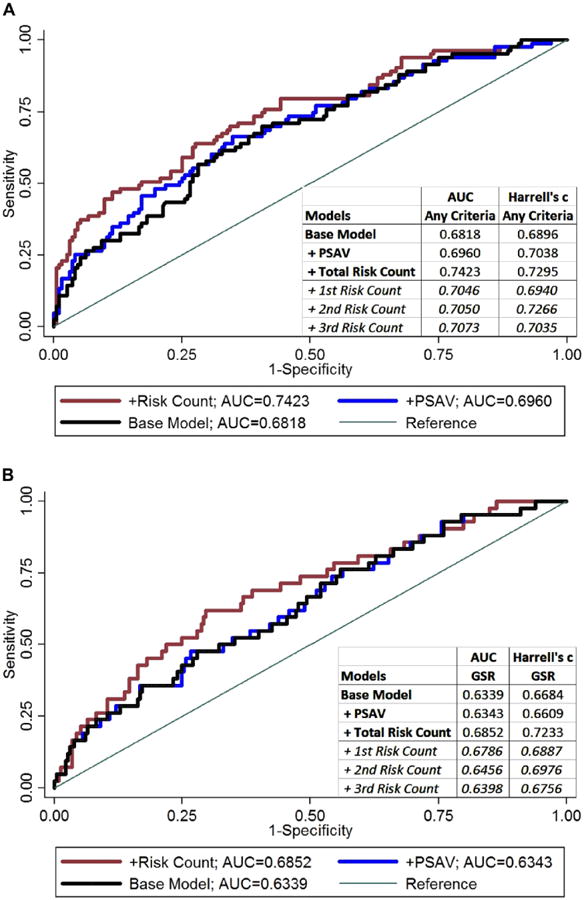
Results: Primary analysis included 275 of 668 men who met very low risk inclusion criteria, of whom 83 (30.2%) were reclassified at a median of 57.1 months. Reclassification risk increased with risk count, that is a risk count of 3 (HR 4.63, 95% CI 1.54-13.87) and 2 (HR 3.73, 95% CI 1.75-7.97) compared to zero. Results were similar for Gleason score reclassification (HR 7.45, 95% CI 1.60-34.71 and 3.96, 95% CI 1.35-11.62, respectively). On secondary analysis the negative predictive value (risk count 1 or less) was 91.5% for reclassification in the next year. Adding the prostate specific antigen velocity risk count improved the AUC in a model including baseline prostate specific antigen density (0.7423 vs 0.6818, p = 0.025) and it outperformed the addition of overall prostate specific antigen velocity (0.7423 vs 0.6960, p = 0.037).
Conclusions: Prostate specific antigen velocity risk count may be useful for monitoring patients on active surveillance and decreasing the frequency of biopsies needed in the long term.
Keywords: biopsy; prostate; prostate-specific antigen; prostatic neoplasms; risk.
Copyright © 2014 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10. - PubMed
-
- Draisma G, Boer R, Otto SJ, et al. Lead times and overdetection due to prostate-specific antigen screening: estimates from the European Randomized Study of Screening for Prostate Cancer. J Natl Cancer Inst. 2003;95:868. - PubMed
-
- Klotz L. Active surveillance: the Canadian experience. Curr Opin Urol. 2012;22:222. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
