

Racial disparities in treatment patterns and clinical outcomes in patients with HER2-positive metastatic breast cancer
- PMID: 24062208
- PMCID: PMC3824350
- DOI: 10.1007/s10549-013-2697-5
Racial disparities in treatment patterns and clinical outcomes in patients with HER2-positive metastatic breast cancer
Abstract
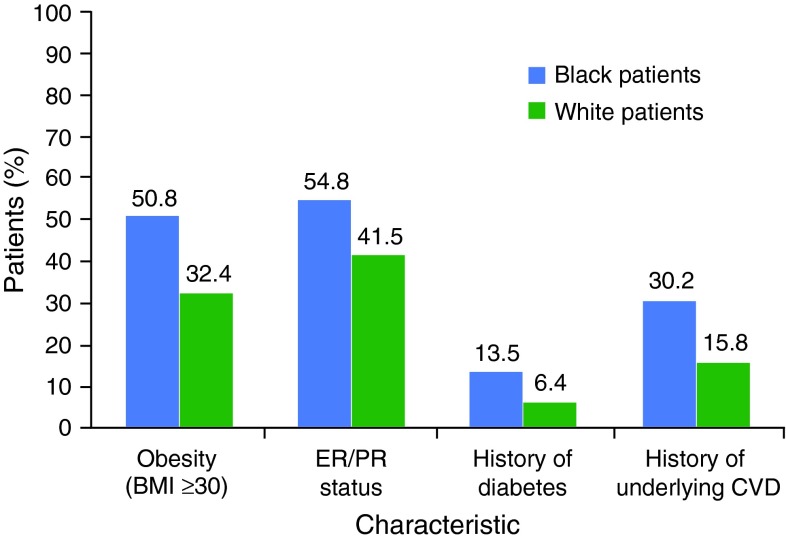
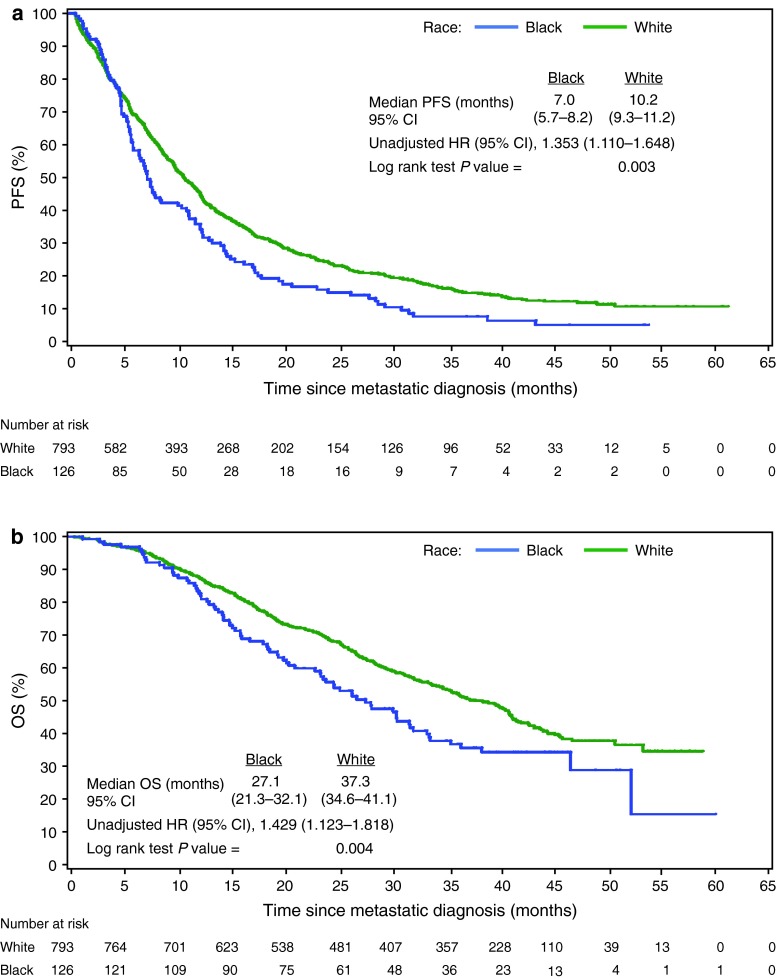
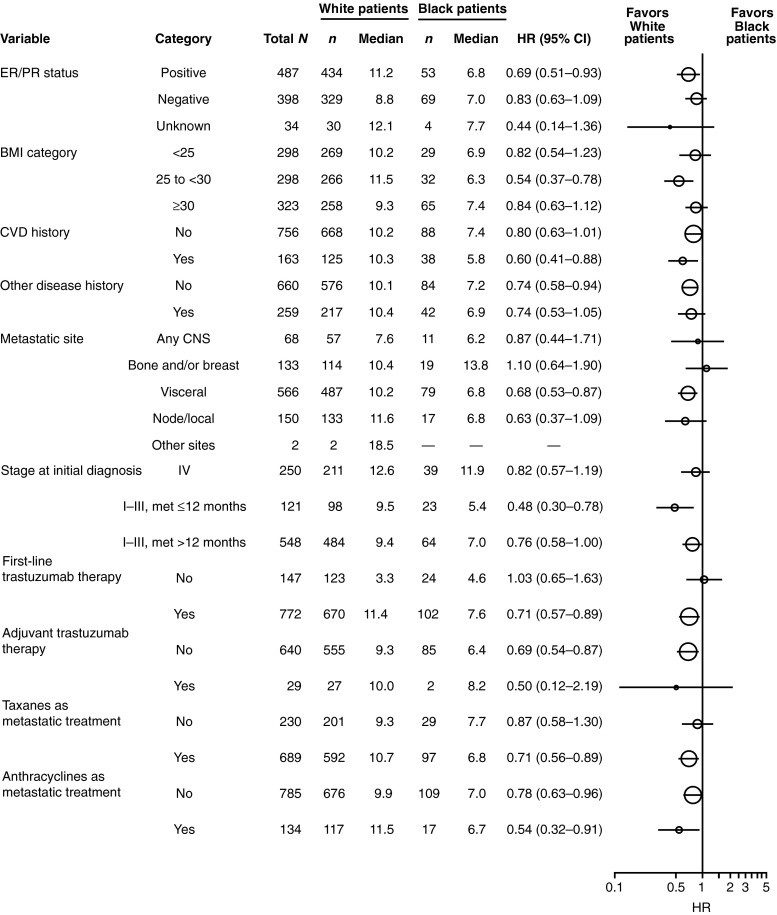
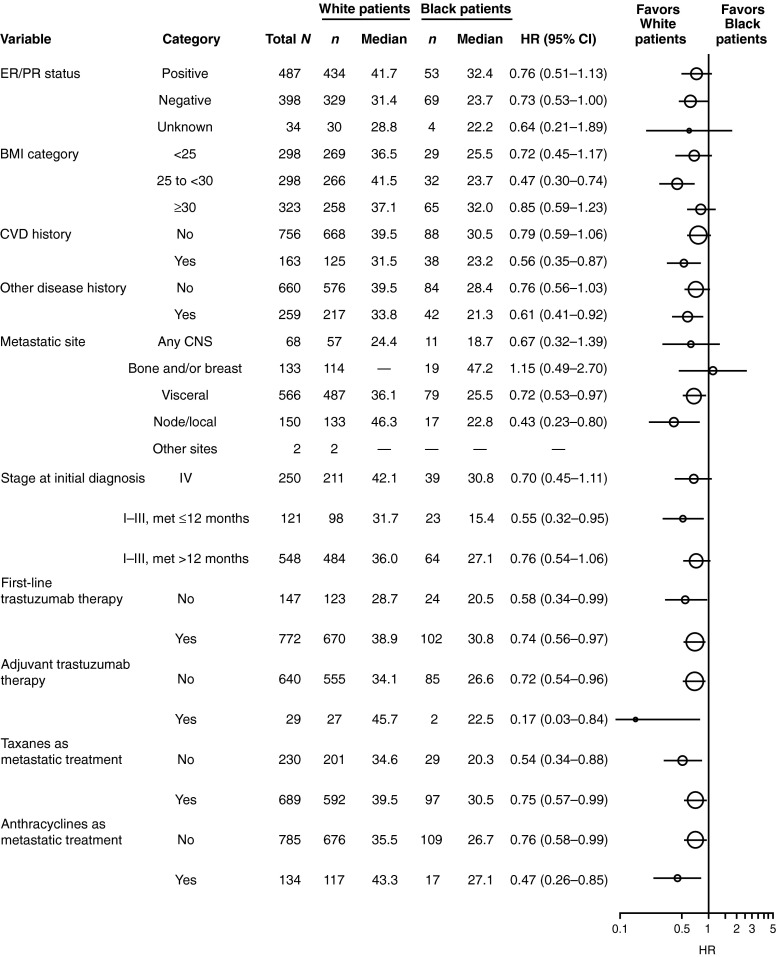
Data characterizing demographics, treatment patterns, and clinical outcomes in black patients with human epidermal growth factor receptor 2 (HER2)-positive metastatic breast cancer (MBC) are limited. registHER is a large, observational cohort study of patients (n = 1,001) with HER2-positive MBC diagnosed ≤6 months of enrollment and followed until death, disenrollment, or June 2009 (median follow-up of 27 months). Demographics, treatment patterns, and clinical outcomes were described for black (n = 126) and white patients (n = 793). Progression-free survival (PFS) following first-line therapy and overall survival (OS) were examined. Multivariate analyses adjusted for baseline and treatment factors. Black patients were more likely than white patients to be obese (body mass index ≥30), to have diabetes, and to have a history of cardiovascular disease; they were also less likely to have estrogen receptor or progesterone receptor positive disease. In patients treated with trastuzumab, the incidence of cardiac safety events (grade ≥3) was higher in black patients (10.9 %) than in white patients (7.9 %). Unadjusted median OS and PFS (months) were significantly lower in black patients than in white patients (OS: black: 27.1, 95 % confidence interval [CI] 21.3-32.1; white: 37.3, 95 % CI 34.6-41.1; PFS: black: 7.0, 95 % CI 5.7-8.2; white: 10.2, 95 % CI 9.3-11.2). The adjusted OS hazard ratio (HR) for black patients compared with white patients was 1.29 (95 % CI 1.00-1.65); adjusted PFS HR was 1.29 (95 % CI 1.05-1.59). This real-world evaluation of a large cohort of patients with HER2-positive MBC shows poorer prognostic factors and independently worse clinical outcomes in black versus white patients. Further research is needed to identify potential biologic differences that could have predictive impact for black patients or that could explain these differences.
Figures
Similar articles
-
First-line treatment patterns and clinical outcomes in patients with HER2-positive and hormone receptor-positive metastatic breast cancer from registHER.Oncologist. 2013;18(5):501-10. doi: 10.1634/theoncologist.2012-0414. Epub 2013 May 7. Oncologist. 2013. PMID: 23652380 Free PMC article. Clinical Trial.
-
Treatment patterns and clinical outcomes in elderly patients with HER2-positive metastatic breast cancer from the registHER observational study.Breast Cancer Res Treat. 2012 Oct;135(3):875-83. doi: 10.1007/s10549-012-2209-z. Epub 2012 Aug 26. Breast Cancer Res Treat. 2012. PMID: 22923238 Free PMC article.
-
Elucidating Determinants of Survival Disparities Among a Real-world Cohort of Metastatic Breast Cancer Patients: A National Cancer Database Analysis.Clin Breast Cancer. 2020 Oct;20(5):e625-e650. doi: 10.1016/j.clbc.2020.04.002. Epub 2020 Apr 18. Clin Breast Cancer. 2020. PMID: 32434711
-
Racial Differences in Breast Cancer Survival Between Black and White Women According to Tumor Subtype: A Systematic Review and Meta-Analysis.J Clin Oncol. 2024 Nov 10;42(32):3867-3879. doi: 10.1200/JCO.23.02311. Epub 2024 Sep 17. J Clin Oncol. 2024. PMID: 39288352
-
Prognostic value of intrinsic subtypes in hormone-receptor-positive metastatic breast cancer: systematic review and meta-analysis.ESMO Open. 2023 Jun;8(3):101214. doi: 10.1016/j.esmoop.2023.101214. Epub 2023 Apr 17. ESMO Open. 2023. PMID: 37075698 Free PMC article.
Cited by
-
Literature review of data-based models for identification of factors associated with racial disparities in breast cancer mortality.Health Syst (Basingstoke). 2018 Mar 11;8(2):75-98. doi: 10.1080/20476965.2018.1440925. eCollection 2019. Health Syst (Basingstoke). 2018. PMID: 31275571 Free PMC article. Review.
-
Racial disparity in breast cancer: can it be mattered for prognosis and therapy.J Cell Commun Signal. 2018 Mar;12(1):119-132. doi: 10.1007/s12079-017-0416-4. Epub 2017 Nov 29. J Cell Commun Signal. 2018. PMID: 29188479 Free PMC article. Review.
-
Untreated head and neck cancer: Natural history and associated factors.Head Neck. 2021 Jan;43(1):89-97. doi: 10.1002/hed.26460. Epub 2020 Sep 11. Head Neck. 2021. PMID: 32914515 Free PMC article.
-
The Impact of Primary Tumor Surgery on Survival in HER2 Positive Stage IV Breast Cancer Patients in the Current Era of Targeted Therapy.Ann Surg Oncol. 2020 Aug;27(8):2711-2720. doi: 10.1245/s10434-020-08310-2. Epub 2020 Mar 10. Ann Surg Oncol. 2020. PMID: 32157524
-
Using Phosphatidylinositol Phosphorylation as Markers for Hyperglycemic Related Breast Cancer.Int J Mol Sci. 2020 Mar 27;21(7):2320. doi: 10.3390/ijms21072320. Int J Mol Sci. 2020. PMID: 32230859 Free PMC article.
References
-
- Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, Conway K, Karaca G, Troester MA, Tse CK, Edmiston S, Deming SL, Geradts J, Cheang MC, Nielsen TO, Moorman PG, Earp HS, Millikan RC. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006;295:2492–2502. doi: 10.1001/jama.295.21.2492. - DOI - PubMed
-
- Huo D, Ikpatt F, Khramtsov A, Dangou JM, Nanda R, Dignam J, Zhang B, Grushko T, Zhang C, Oluwasola O, Malaka D, Malami S, Odetunde A, Adeoye AO, Iyare F, Falusi A, Perou CM, Olopade OI. Population differences in breast cancer: survey in indigenous African women reveals over-representation of triple-negative breast cancer. J Clin Oncol. 2009;27:4515–4521. doi: 10.1200/JCO.2008.19.6873. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
