

Marital status and survival in patients with cancer
- PMID: 24062405
- PMCID: PMC4878087
- DOI: 10.1200/JCO.2013.49.6489
Marital status and survival in patients with cancer
Abstract
Purpose: To examine the impact of marital status on stage at diagnosis, use of definitive therapy, and cancer-specific mortality among each of the 10 leading causes of cancer-related death in the United States.
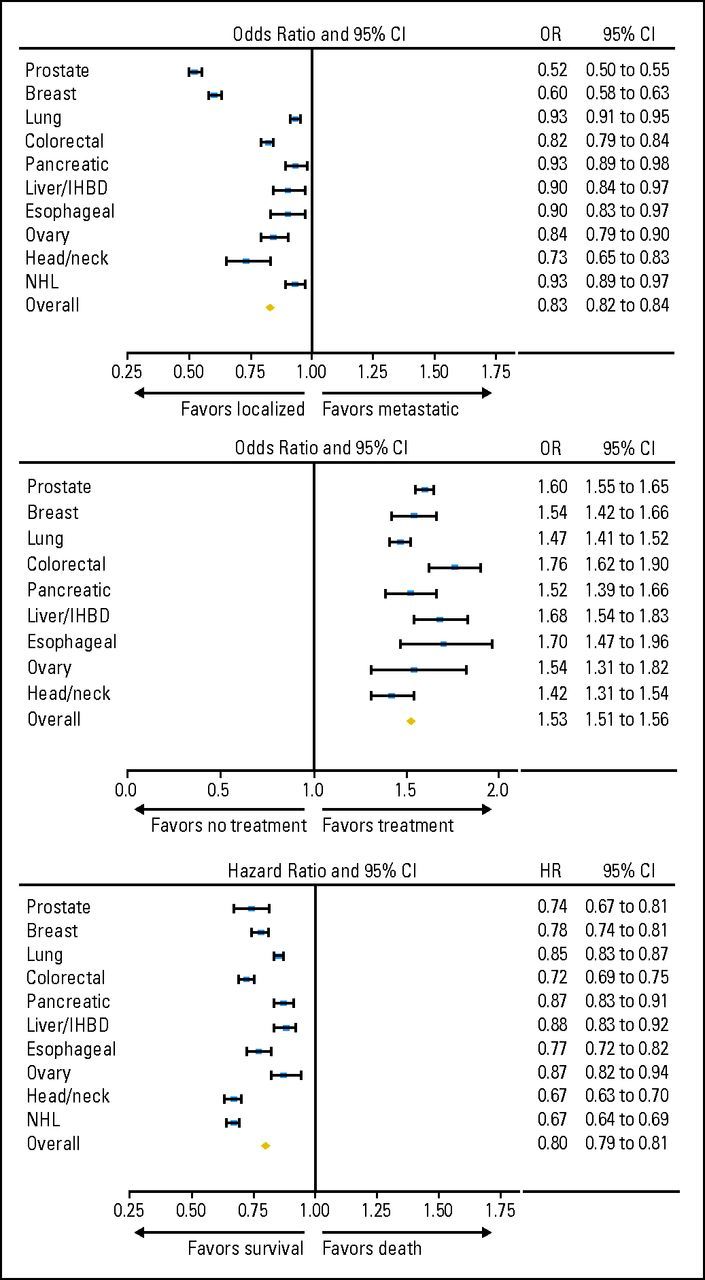
Methods: We used the Surveillance, Epidemiology and End Results program to identify 1,260,898 patients diagnosed in 2004 through 2008 with lung, colorectal, breast, pancreatic, prostate, liver/intrahepatic bile duct, non-Hodgkin lymphoma, head/neck, ovarian, or esophageal cancer. We used multivariable logistic and Cox regression to analyze the 734,889 patients who had clinical and follow-up information available.
Results: Married patients were less likely to present with metastatic disease (adjusted odds ratio [OR], 0.83; 95% CI, 0.82 to 0.84; P < .001), more likely to receive definitive therapy (adjusted OR, 1.53; 95% CI, 1.51 to 1.56; P < .001), and less likely to die as a result of their cancer after adjusting for demographics, stage, and treatment (adjusted hazard ratio, 0.80; 95% CI, 0.79 to 0.81; P < .001) than unmarried patients. These associations remained significant when each individual cancer was analyzed (P < .05 for all end points for each malignancy). The benefit associated with marriage was greater in males than females for all outcome measures analyzed (P < .001 in all cases). For prostate, breast, colorectal, esophageal, and head/neck cancers, the survival benefit associated with marriage was larger than the published survival benefit of chemotherapy.
Conclusion: Even after adjusting for known confounders, unmarried patients are at significantly higher risk of presentation with metastatic cancer, undertreatment, and death resulting from their cancer. This study highlights the potentially significant impact that social support can have on cancer detection, treatment, and survival.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Marriage is as protective as chemotherapy in cancer care.J Clin Oncol. 2013 Nov 1;31(31):3852-3. doi: 10.1200/JCO.2013.51.5080. Epub 2013 Sep 23. J Clin Oncol. 2013. PMID: 24062396 No abstract available.
-
Reply to M.G. Bare et al.J Clin Oncol. 2014 Jul 10;32(20):2184. doi: 10.1200/JCO.2014.55.6688. Epub 2014 Jun 2. J Clin Oncol. 2014. PMID: 24888805 No abstract available.
-
Omission of sexual and gender minority patients.J Clin Oncol. 2014 Jul 10;32(20):2182-3. doi: 10.1200/JCO.2014.55.6126. Epub 2014 Jun 2. J Clin Oncol. 2014. PMID: 24888807 No abstract available.
-
Re: marital status and survival in patients with cancer.J Urol. 2014 Jun;191(6):1783-4. doi: 10.1016/j.juro.2014.03.064. Epub 2014 Mar 20. J Urol. 2014. PMID: 25280281 No abstract available.
References
-
- Pew Research Center. Social and demographic trends. http://www.pewsocialtrends.org.
-
- Fosså SD, Cvancarova M, Chen L, et al. Adverse prognostic factors for testicular cancer-specific survival: A population-based study of 27,948 patients. J Clin Oncol. 2011;29:963–970. - PubMed
-
- Rendall MS, Weden MM, Favreault MM, et al. The protective effect of marriage for survival: A review and update. Demography. 2011;48:481–506. - PubMed
-
- Sammon JD, Morgan M, Djahangirian O, et al. Marital status: A gender-independent risk factor for poorer survival after radical cystectomy. BJU Int. 2012;110:1301–1309. - PubMed
-
- Wang L, Wilson SE, Stewart DB, et al. Marital status and colon cancer outcomes in US Surveillance, Epidemiology and End Results registries: Does marriage affect cancer survival by gender and stage? Cancer Epidemiol. 2011;35:417–422. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
